![]()
![]()
Ilyas KayaciogluI; Ahmet Can TopcuI; Kamile OzerenI; Yasin OzdenI; Ahmet BolukcuI; Mehmet YildirimII
DOI: 10.21470/1678-9741-2018-0055
CABG = Coronary artery bypass grafting
CPB = Cardiopulmonary bypass
CT = Computed tomography
Cx = Circumflex
FEV1 = Forced expiratory volume in 1st second
FVC = Forced vital capacity
LAD = Left anterior descending
LITA = Left internal thoracic artery
MRI = Magnetic resonance imaging
INTRODUCTION
Significant anatomical and functional changes occur following pneumonectomy. Mediastinal structures displace toward the side of the resected lung, pulmonary reserve is reduced, and the remaining lung compensatorily enlarges and herniates over the midline with elevation of the diaphragm[1,2]. Owing to these changes, surgical access to the heart and great vessels becomes challenging, and there is an increased risk of postoperative pulmonary complications.
CASE REPORT
A 24-year-old female patient presented to our clinic with dyspnea. She had undergone a left pneumonectomy for advanced and complicated bronchiectasis 10 years ago.
Clinical Findings
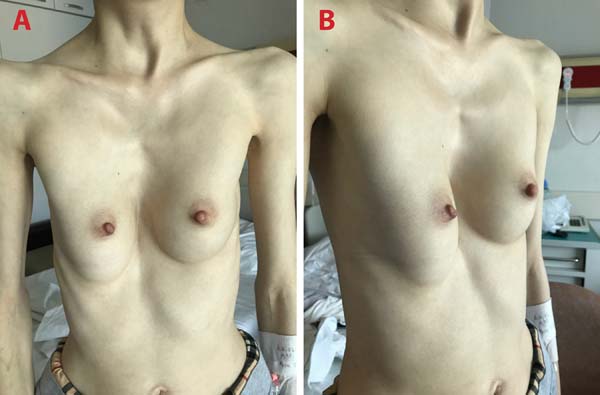
She had marfanoid habitus, pectus excavatum, scoliosis, and a grade 4, pansystolic, high-pitched, blowing murmur best heard at the right sternal border (Figures 1A and B).
Diagnostic Assessment
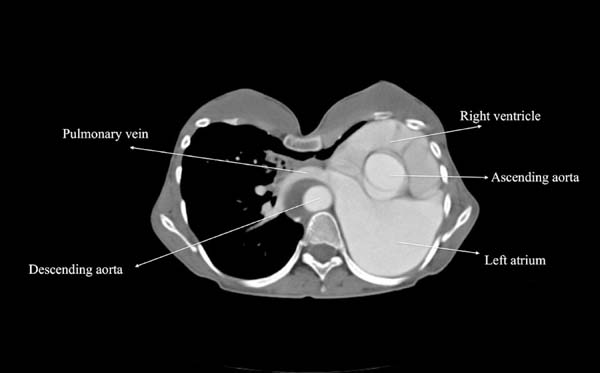
Transthoracic echocardiogram revealed severe mitral regurgitation due to myxomatous mitral valve with bileaflet prolapse and chordal elongation, secondary pulmonary hypertension, and tricuspid regurgitation with a dilated right atrium. Her ejection fraction was 35%, left ventricle end-diastolic diameter was 72 mm, and end-systolic diameter was 59 mm. She also had a borderline ascending aortic aneurysm measuring 40 mm in diameter. Pulmonary function test demonstrated reduced forced vital capacity (FVC), 1.11 L (31.7% of predicted), and reduced forced expiratory volume in 1st second (FEV1), 1.05 L (34.6% of predicted). A contrast-enhanced computed tomography (CT) scan was performed to examine the mediastinal structures and alternative cannulation sites (Figure 2). Heart and great vessels were displaced to the left, and the right lung was enlarged and crossing the midline, anterior to the heart. The proxymal ascending aorta was 40 mm in diameter. Additionally, a chronic type B aortic dissection was present. CT scan revealed that the ascending aorta and the superior and inferior venae cavae were suitable for cannulation.
Therapeutic Intervention
The patient received intensive chest physiotherapy before surgery to reduce postoperative pulmonary complications.
A vertical midline incision on skin, subcutaneous tissues, and pectoralis fascia was made over the sternum. Following elevation of pectoralis muscles from the anterior chest wall, a median sternotomy was performed. Costal cartilages of the 3rd to 8th ribs were removed. The right lung was retracted from the midline. Cardiopulmonary bypass (CPB) was initiated via ascending aortic and bicaval cannulation, and cardiac arrest was obtained. We did not use topical cardiac hypothermia to prevent phrenic nerve injury. Both atria were relatively easy to expose due to leftward shift and rotation of the heart. A mitral valve replacement and a tricuspid ring annuloplasty was performed using biatrial approach. CPB was terminated. A bar was placed behind the sternum and fixed to the pectoralis muscle fibers bilaterally. After completion of the Ravitch procedure, the sternum was closed. The patient was transferred to a dedicated cardiac surgery intensive care unit and she was successfully extubated at the postoperative 6th hour. Her recovery was uneventful and she was discharged on postoperative day 9 (Figures 3A and B).
Follow-up and Outcomes
The patient remains symptom-free 3 months after surgery and she is scheduled to have a bar removal 3 months later (Figures 4A and B).
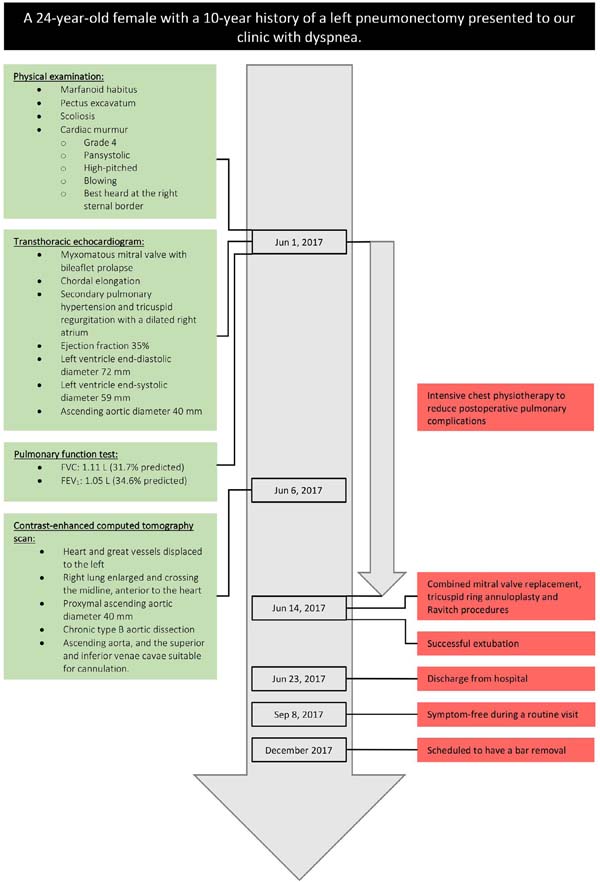
The Figure 5 presents a timeline of interventions and outcomes.
DISCUSSION
After conducting a Medline search from 1966 to April 2018 using the search terms "pneumonectomy" and "open heart surgery" or "coronary artery bypass" or "mitral valve" or "aortic valve" or "revascularization", we identified 30 articles in English language[3-34]. A total of 42 cardiac operations were performed on 38 patients, including the current one (Table 1). The mean patient age was 65.2 years (range: 24-83 years). Twenty-one (76.3%) patients were male. There were 20 (47.6%) isolated coronary artery bypass grafting (CABG) procedures, 18 (42.8%) valvular procedures, and 4 (9.5%) combined CABG and valvular procedures. Two of these operations were transapical aortic valve implantation procedures (patients 29 and 30)[26,27].
| Patient no. |
Author | Publication year |
Sex | Age | Pneumonectomy site |
Years elapsed after pneumonectomy |
Indication for pneumonectomy |
Preoperative data | Operation | Operative details | Complications | Length
of hospital stay (days) |
|
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FEV1 (percent of predicted value) |
FVC (percent of predicted value) |
||||||||||||
| 1 | Berrizbeitia et al.[3] | 1994 | M | 61 | Right | 42 | Bronchiectasis | 21 | 32 | CABG | - 3 SVGs to LAD, OMB, and PDA - Median sternotomy - On-pump | None | 8 |
| 2 | Shibata et al.[4] | 1994 | M | 67 | Left | 13 | Cancer | 77 | 55 | CABG | - 3 SVGs - Median sternotomy - On-pump | None | 57 |
| 3 | Medalion et al.[5] | 1994 | F | 70 | Left | 40 | Tuberculosis | 45 | 52 | CABG | - LITA and 3 SVGs - Median sternotomy - On-pump | None | 11 |
| 4 | Demirtas et al.[6] | 1995 | M | 63 | Left | 20 | Cancer | 36 | 36 | CABG | - LITA and SVG to LAD and OMB - Median sternotomy - On-pump | Prolonged inotropic support, low cardiac output requiring intra-aortic balloon pump insertion, right-sided pneumothorax requiring re-intubation and chest tube insertion, mediastinitis and sternal detachment requiring re-operation, sepsis, and death | 12 |
| 5 | Izzat et al.[7] | 1995 | M | 65 | Right | 10 | Cancer | N/A | N/A | Mitral valve replacement | - Approach to mitral valve through left atrial appendage - Median sternotomy - On-pump | None | 7 |
| 6 | Soltanian et al.[8] | 1998 | F | 70 | Left | 19 | Cancer | N/A | N/A | CABG | - SVG to LAD - Left thoracotomy - Off-pump | None | 7 |
| 7 | Lippmann and Au[9] | 2000 | M | 68 | Left | 15 | Cancer | 56 | 60 | CABG | - SVGs - Median sternotomy - On-pump | Bronchopneumonia, pulmonary embolism, respiratory failure requiring re-intubation, and death | 6 |
| 8 | M | 73 | Left | 22 | Cancer | 53 | 58 | CABG | - LITA and SVGs - Median sternotomy - On-pump | Postoperative bleeding requiring re-exploration, atrial fibrillation, hemothorax requiring re-intubation, and chest tube insertion | 48 | ||
| 9 | Gölbasi et al.[10] | 2001 | M | 58 | Right | 0.75 | Cancer | 50 | 44 | CABG | - SVGs to LAD, OMB, and RCA - Median sternotomy - On-pump | None | 9 |
| 10 | Diab et al.[11], Jamaleddine and Obeid[12] | 2001 | M | 64 | Right | 6 | Trauma | N/A | N/A | CABG | - SVGs to LAD, Cx, and RCA - Median sternotomy - On-pump | Respiratory failure requiring re-intubation | 12 |
| 11 | El-Hamamsy et al.[13] | 2003 | F | 65 | Right | 51 | Tuberculosis | 36 | 44 | Mitral valve replacement and tricuspid valve annuloplasty | - Standard left atrial approach - Median sternotomy - On-pump | Pneumothorax requiring chest tube insertion | 20 |
| 12 | F | 71 | Right | 50 | Tuberculosis | 28 | 27 | CABG | - 3 SVGs - Median sternotomy - Off-pump | None | 6 | ||
| 13 | Kumar et al.[14] | 2003 | M | 70 | Left | 15 | Cancer | N/A | N/A | CABG | - LITA and SVG to LAD and PDA - Median sternotomy - Off-pump | None | 7 |
| 14 | Erdil et al.[15] | 2004 | M | 51 | Right | 17 | Tuberculosis | 45 | 43 | CABG | - 2 RAs to LAD, OMB, and RCA - Median sternotomy - On-pump | None | 5 |
| 15 | Shanker et al.[16] | 2005 | M | 80 | Left | 27 | Cancer | 46 | N/A | CABG, mitral valve repair, and aortic valve replacement | - 1 SVG to LAD and diagonal artery - Approach to both valves via aortotomy - Bioprosthetic aortic valve - Median sternotomy - On-pump | None | 10 |
| 16 | Bernet et al.[17] | 2006 | M | 58 | Right | 3 | Cancer | 59 | 59 | CABG | - LITA and SVG to LAD and OMB - Median sternotomy - Off-pump | None | 8 |
| 17 | Hukusi Us et al.[18] | 2006 | M | 74 | Left | 15 | Cancer | 45 | 60 | CABG | - LITA and SVG to LAD, Cx, and RCA - Median sternotomy - On-pump | None | 7 |
| 18 | Stoller et al.[19] | 2007 | F | 54 | Left | 3 | Cancer | 61 | 61 | CABG | - SVGs to LAD and Cx - Left thoracotomy - Off-pump | None | 5 |
| 19 | M | 48 | Left | 18 | Cancer | N/A | N/A | CABG | - 3 SVGs to LAD, Cx, and RCA - Median sternotomy - On-pump | Respiratory failure requiring prolonged mechanical ventilation and extracorporeal membrane oxygenation and pneumonia | 26 | ||
| 26 | 37 | 42 | Mitral and tricuspid valve repair | - Right atriotomy and transseptal approach - Re-sternotomy - On-pump, deep hypothermic circulatory arrest | Atrial fibrillation | 13 | |||||||
| 20 | M | 71 | Left | 7 | Cancer | 33 | 40 | Mitral valve replacement and tricuspid valve annuloplasty | - Right atriotomy and transseptal approach - Median sternotomy - On-pump | Renal failure and atrial fibrillation | N/A | ||
| 21 | F | 74 | Left | 37 | Cancer | 75 | 70 | CABG | - 4 SVGs to LAD, OMBs, and RCA - Left thoracotomy - On-pump | None | 6 | ||
| 22 | Sleilaty et al.[20] | 2007 | M | 71 | Right | 20 | Trauma | 53 | 48 | CABG and aortic valve replacement | - SVG to diagonal artery - Bioprosthetic aortic valve - Median sternotomy - On-pump | None | 13 |
| 23 | Barreda et al.[21] | 2008 | M | 68 | Left | 4 | Cancer | N/A | N/A | Aortic valve replacement | - Left anterior thoracotomy - On-pump | Re-exploration for worsening of preoperative mitral insufficiency due to leaflet tethering 1 day after aortic valve replacement | N/A |
| Mitral valve annuloplasty | - Left posterior thoracotomy - On-pump | ||||||||||||
| 24 | Ghotkar et al.[22] | 2008 | M | 71 | Left | 18 | Cancer | 42 | 53 | CABG | - SVG to LAD and PDA - Median sternotomy - On-pump | Postoperative bleeding requiring re-exploration and atrial fibrillation | 17 |
| 25 | F | 77 | Right | 1 | Cancer | 64 | 63 | Aortic valve replacement | - Bioprosthetic aortic valve | None | N/A | ||
| 26 | Zhao et al.[23] | 2008 | M | 57 | Left | 7 | Cancer | 61.9 | 70.3 | CABG | - 2 SVGs to LAD, RCA, and OMB - Left posterolateral thoracotomy - Off-pump | None | 9 |
| 27 | Us et al. [24] | 2010 | M | 65 | Left | 8 | N/A | 45 | 50 | Mitral valve replacement and subaortic membrane resection | - transseptal approach and aortotomy - mechanical mitral valve prosthesis - median sternotomy - on-pump | None | 7 |
| 28 | Stamou et al. [25] | 2010 | M | 83 | Left | 8 | Cancer | 48 | N/A | CABG and aortic valve replacement | - left anterolateral thoracotomy - on-pump | None | 5 |
| 29 | Ferrari et al. [26] | 2011 | M | 64 | Left | 8 | Cancer | N/A | N/A | Transapical aortic valve implantation | - left anterolateral thoracotomy - off-pump | None | N/A |
| 30 | Raja et al. [27] | 2011 | F | 67 | Right | 18 | Cancer | 49 | N/A | Transapical aortic valve implantation | - right anterior thoracotomy - off-pump | None | 4 |
| 31 | Ushijima et al. [28] | 2011 | M | 82 | Left | 20 | Cancer | 63.8 | 63.8 | CABG | - LITA, RA and RGEA to LAD, PL and PDA - left thoracotomy - off-pump | None | N/A |
| 32 | Wilhelmi et al. [29] | 2013 | M | 68 | Right | 8 | Cancer | 56 | 58 | Aortic valve replacement | - bioprosthetic aortic valve - right anterolateral thoracotomy - on-pump | None | 6 |
| 33 | Dag et al. [30] | 2013 | M | 72 | Left | 13 | Cancer | N/A | N/A | CABG and mitral valve replacement | - SVG to LAD and RCA - standard left atrial approach - mechanical mitral valve prosthesis - median sternotomy - on-pump | None | N/A |
| 34 | Gennari et al. [31] | 2014 | M | 71 | Left | 4 | Cancer | 53 | 54 | Mitral and tricuspid valve repair | - median sternotomy - on-pump | None | 11 |
| 35 | Rose et al. [32] | 2015 | M | 31 | Right | 8 | Cancer | N/A | N/A | Mitral valve repair | - left atrial approach - video-assisted right thoracotomy - on-pump | None | 8 |
| 36 | Takahashi et al. [33] | 2016 | M | 72 | Right | 32 | Tuberculosis | N/A | N/A | Mitral valve replacement | - Right thoracotomy - on-pump | Periprosthetic leak | N/A |
| 32 | N/A | N/A | Repair of mitral peri-prosthetic leak (2 months after valve replacement) | - Right thoracotomy - on-pump | None | N/A | |||||||
| 40 | N/A | N/A | Repair of mitral peri-prosthetic leak (8 years after valve replacement) | - Cranial-sided approach to left atrium - median sternotomy - on-pump | None | N/A | |||||||
| 37 | Sinha et al. [34] | 2016 | M | 61 | Right | 47 | Scimitar syndrome | N/A | N/A | Mitral valve repair | - left atrial approach - video-assisted right thoracotomy - on-pump | None | 5 |
| 38 | Current patient | 2018 | F | 24 | Left | 10 | Bronchiectasis | 34.6 | 31.7 | Mitral valve replacement and tricuspid valve annuloplasty | - standard left atrial approach - median sternotomy combined with Ravitch procedure - on-pump | None | 9 |
CABG=Coronary artery bypass grafting; Cx=circumflex; FEV1=forced expiratory volume in 1st second; FVC=forced vital capacity; LAD=left anterior descending; LITA=left internal thoracic artery; OMB=obtuse marginal branch; PDA=posterior descending artery; RAs=radial arteries; RCA=right coronary artery; SVG=saphenous vein graft

Fifteen (39.4%) patients had a previous right pneumonectomy. The most common indication for pneumonectomy was cancer (n=27, 71%), followed by tuberculosis (n=5, 13.1%), trauma (n=2, 5.2%), bronchiectasis (n=2, 5.2%), scimitar syndrome (n=1, 2.6%), and unknown etiology (n=1, 2.6%). Preoperative FEV1 values were available for 28 patients and averaged 49% of predicted (range: 21-77%). Preoperative FVC values were available for 25 patients and averaged 49.2% of predicted (range: 27-70.3%).
The preferred surgical incision was a median sternotomy in 26 (61.9%) cases, a left thoracotomy in 9 (21.4%) cases, a right thoracotomy in 6 (14.2%) cases, and it was not specified in 1 (2.3%) case. Patients 35 and 37 underwent surgery utilizing video-assisted right thoracotomy[32,34]. Among 24 CABG operations, a left internal thoracic artery was used as a bypass conduit in 7 (29.1%) cases. The use of a right internal thoracic artery was not reported. Complete arterial revascularization was performed in 2 (8.3%) cases. Among 20 isolated CABG operations, 7 (35%) were carried out without the use of CPB.
Length of hospital stay data was available in 32 cases and averaged 12 days (range: 4-57 days). Postoperative complications were experienced after 11 (26.1%) operations. The most common complication was atrial fibrillation (n=5, 11.9%), followed by respiratory failure requiring re-intubation (n=4, 9.5%), pneumothorax (n=2, 4.7%), pneumonia (n=2, 4.7%), and bleeding requiring re-exploration (n=2, 4.7%). Two (5.2%) patients did not survive to discharge.
Previous pneumonectomy adds two major risks to cardiac operations: (1) there is an increased risk of postoperative pulmonary complications due to reduced lung capacity; (2) heart and great vessels are displaced and rotated, making surgical exposure more difficult.
Six months after pneumonectomy, FVC decreases by 36% and FEV1 by 34%. These parameters do not significantly improve beyond 6 months[2]. Considering that the pulmonary function may deteriorate significantly after cardiac surgery even in patients who have normal preoperative respiratory function, previous pneumonectomy poses a great risk of postoperative pulmonary complications[35]. Hulzebos et al.[36] found preoperative inspiratory muscle training to be effective in preventing postoperative pulmonary complications in high-risk patients undergoing elective CABG surgery. Conventional measures such as avoidance of phrenic nerve injury and fluid overload, early extubation, early mobilization, and postoperative chest physiotherapy should be utilized. Central venous line should be placed on the side of the pneumonectomy to avoid pneumothorax.
Considerable anatomical changes occur in long-term survivors after pneumonectomy. Smulders et al.[1] evaluated the function and position of the heart using dynamic magnetic resonance imaging (MRI) in 15 patients who underwent pneumonectomy at least 5 years ago. They reported that although varying degrees of mediastinal shift occur in all patients, right-sided pneumonectomy is mostly associated with a lateral shift and only a minor rotation, whereas left-sided pneumonectomy leads to a greater degree of rotation[1]. Whether the patient had a left or right pneumonectomy, it affects the choice of surgical approach. For instance, in the case of a previous left pneumonectomy, it may be easier to bypass left-sided coronary arteries through a left thoracotomy, rather than a median sternotomy, and mitral and tricuspid valves may be inaccessible from the usual right thoracotomy. Stoller et al.[19] reported difficult exposure of the mitral valve through a median sternotomy in a patient who underwent a left pneumonectomy 9 years ago. However, we found it relatively easy to perform a mitral valve surgery in a similar setting. Because long-term anatomical changes after pneumonectomy vary considerably among patients, preoperative CT and/or MRI should be performed to assess the exact locations of cardiac structures and cannulation sites[37]. Decision of surgical approach should only be made after carefully examining the extent of the shift and the rotation of the cardiac structures.
Another subject that needs addressing is the concomitant pectus excavatum. Schmidt et al.[38] advocate simultaneous correction of the pectus excavatum in patients requiring cardiac surgery. We resected deformed cartilages prior to sternotomy to improve surgical exposure as previously reported by Sacco-Casamassima et al.[39].
Cardiac operations on patients with previous pneumonectomy can be performed with a favourable outcome. Thorough preoperative evaluation with imaging studies to assess cardiac position and function and intensive respiratory physiotherapy are essential.
REFERENCES
1. Smulders SA, Holverda S, Vonk-Noordegraaf A, van den Bosch HC, PostJC, Marcus JT, et al. Cardiac function and position more than 5 years afterpneumonectomy. Ann Thorac Surg. 2007;83(6):1986-92.
2. Bolliger CT, Jordan P, Solèr M, Stulz P, Tamm M, Wyser C, et al.Pulmonary function and exercise capacity after lung resection. Eur Respir J.1996;9(3):415-21.
3. Berrizbeitia LD, Anderson WA, Laub GW, McGrath LB. Coronary arterybypass grafting after pneumonectomy. Ann Thorac Surg.1994;58(5):1538-40.
4. Shibata T, Suehiro S, Kimura E, Nishizawa H, Minamimura H, KinoshitaH. Coronary artery bypass grafting 13 years after pneumonectomy. Nihon KyobuGeka Gakkai Zasshi. 1994;42(7):1105-7.
5. Medalion B, Elami A, Milgalter E, Merin G. Open heart operationafter pneumonectomy. Ann Thorac Surg. 1994;58(3):882-4.
6. Demirtas MM, Akar H, Kaplan M, Dagsali S. Coronary artery bypassoperation after pneumonectomy. Ann Thorac Surg.1995;60(1):232-3.
7. Izzat MB, Regragui IA, Angelini GD. Mitral valve replacement afterprevious right pneumonectomy. Ann Thorac Surg.1995;59(1):222-4.
8. Soltanian H, Sanders JH Jr, Robb JC, Marrin CA. Hybrid myocardialrevascularization after previous left pneumonectomy. Ann Thorac Surg.1998;65(1):259-60.
9. Lippmann M, Au J. Coronary artery bypass surgery after previouspneumonectomy: two case reports. Scand Cardiovasc J.2000;34(5):541-2.
10. Gölbasi I, Türkay C, Sahin N, Oz N, Akbulut E, Gülmez H, et al.Coronary artery bypass grafting nine months after pneumonectomy. Tex Heart InstJ. 2001;28(2):146-8.
11. Diab KA, Khatib MF, Obeid M, Jamaleddine GW. Coronary artery bypassgrafting after pneumonectomy. Eur J Cardiothorac Surg.2001;19(3):362-4.
12. Jamaleddine GW, Obeid M. Reply to Pezzella. Eur J Cardiothorac Surg.2001;20:1274.
13. El-Hamamsy I, Stevens LM, Perrault LP, Carrier M. Rightpneumonectomy and thoracoplasty followed by coronary artery bypass grafting andmitral valve replacement. J Thorac Cardiovasc Surg.2003;125(1):215-6.
14. Kumar P, Swift SJ, Athanasiou T, Nelson JS, Glenville B. CABG15-years after left pneumonectomy: feasibility of off-pump approach. CardiovascSurg. 2003;11(4):305-7.
15. Erdil N, Nisanoglu V, Toprak HI, Erdil FA, Kuzucu A, Battaloglu B.Arterial myocardial revascularization using bilateral radial artery 17 yearsafter right pneumonectomy. Tex Heart Inst J. 2004;31(1):96-8.
16. Shanker VR, Yadav S, Hodge AJ. Coronary artery bypass grafting withvalvular heart surgery after pneumonectomy. ANZ J Surg.2005;75(1-2):88-90. [MedLine]
17. Bernet FH, Reineke DC, Grapow MT, Zerkowski HR. OPCAB surgery afterright pneumonectomy. J Card Surg. 2006;21(1):92-3.
18. Hulusi Us M, Arslan Y, Ozbek C, Basaran M, Yidiz Y, Ogus T, et al.Coronary artery bypass grafting after left pneumonectomy. J Cardiothorac VascAnesth. 2006;20(5):709-11.
19. Stoller JK, Blackstone E, Petterson G, Mihaljevic T. Coronary arterybypass graft and/or valvular operations following prior pneumonectomy: report offour new patients and review of the literature. Chest.2007;132(1):295-301. [MedLine]
20. Sleilaty G, Yazigi A, El Asmar B, Hajj-Chahine J, Nakad J,Madi-Jebara S, et al. Combined coronary surgery and aortic valve replacementafter previous right pneumonectomy. J Med Liban.2007;55(2):101-3.
21. Barreda T, Laali M, Dorent R, Acar C. Left thoracotomy for aorticand mitral valve surgery in a case of mediastinal displacement due topneumonectomy. J Heart Valve Dis. 2008;17(2):239-42.
22. Ghotkar SV, Aerra V, Mediratta N. Cardiac surgery in patients withprevious pneumonectomy. J Cardiothorac Surg. 2008;3:11.
23. Zhao BQ, Chen RK, Song JP. Coronary artery bypass grafting afterpneumonectomy. Tex Heart Inst J. 2008;35(4):470-1.
24. Us MH, Ugurlucan M, Basaran M, Selimoglu O, Kocailik A. Mitral valvereplacement and subaortic membrane resection following pneumonectomy. Case RepMed. 2010;2010:480703.
25. Stamou SC, Murphy MC, Kouchoukos NT. Aortic valve replacement andcoronary artery bypass via left anterior thoracotomy after previous leftpneumonectomy. J Thorac Cardiovasc Surg. 2010;140(3):719-20.
26. Ferrari E, Sulzer C, Marcucci C, Qanadly SD, Locca D, Berdajs D, etal. Transapical aortic valve implantation following left pneumonectomy. J CardSurg. 2011;26(1):28-30. [MedLine]
27. Raja Y, Mascaro J, Doshi SN. Successful implantation of the EdwardsSapien THV via direct aortic access in a patient with previous pneumonectomy andno other access. Catheter Cardiovasc Interv.2011;78(7):1008-12.
28. Ushijima T, Kikuchi Y, Ikeda C, Takata M, Yamamoto Y, Watanabe G.Totally arterial off-pump coronary artery bypass grafting after pneumonectomy.Ann Thorac Cardiovasc Surg. 2011;17(3):320-2.
29. Wilhelmi M, Rodt T, Ismail I, Haverich A. Aortic valve replacementvia right anterolateral thoracotomy in the case of a patient with extrememediastinal right-shift following pneumonectomy. J Cardiothorac Surg.2013;8:20.
30. Dag O, Kaygin MA, Arslan U, Kiymaz A, Kahraman N, Erkut B. Mitralvalve and coronary artery bypass surgeries 13 years after pneumonectomy for lungcancer. Cardiovasc J Afr. 2013;24(8):e1-4.
31. Gennari M, Kassem S, Teruzzi G, Agrifoglio M. Coronary arterydisease associated with severe mitral and tricuspid valve regurgitation afterleft pneumonectomy: report of a successful hybrid procedure. Interact CardiovascThorac Surg. 2014;19(2):318-20.
32. Rose D, Liew CK, Zacharias J. Mitral valve repair after a rightpneumonectomy: a minimally invasive approach. Interact Cardiovasc Thorac Surg.2015;21(4):551-3.
33. Takahashi Y, Shibata T, Sasaki Y, Kato Y, Motoki M, Morisaki A, etal. A cranial-sided approach for repeated mitral periprosthetic leak after rightpneumonectomy. Ann Thorac Surg. 2016;101(3):1174-6.
34. Sinha S, Morgan-Hughes N, O'Toole L, Hunter S. Minimal access mitralvalve repair in a patient with a right pneumonectomy for Scimitar syndrome.Interact Cardiovasc Thorac Surg. 2016;22(6):851-3.
35. Westerdahl E, Lindmark B, Bryngelsson I, Tenling A. Pulmonaryfunction 4 months after coronary artery bypass graft surgery. Respir Med.2003;97(4):317-22.
36. Hulzebos EH, Helders PJ, Favié NJ, De Bie RA, Brutel de la RiviereA, Van Meeteren NL. Preoperative intensive inspiratory muscle training toprevent postoperative pulmonary complications in high-risk patients undergoingCABG surgery: a randomized clinical trial. JAMA.2006;296(15):1851-7.
37. Kopec SE, Irwin RS, Umali-Torres CB, Balikian JP, Conlan AA. Thepostpneumonectomy state. Chest. 1998;114(4):1158-84.
38. Schmidt J, Redwan B, Koesek V, Aebert H, Tjan TD, Martens S, et al.Pectus excavatum and cardiac surgery: simultaneous correction advocated. ThoracCardiovasc Surg. 2014;62(3):238-44.
39. Sacco-Casamassima MG, Wong LL, Papandria D, Abdullah F, Vricella LA,Cameron DE, et al. Modified Nuss procedure in concurrent repair of pectusexcavatum and open heart surgery. Ann Thorac Surg.2013;95(3):1043-9.
No financial support.
No conflict of interest.
Authors' roles & responsibilities
IK Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published
ACT Substantial contributions to the conception or design of the work; final approval of the version to be published
KO Substantial contributions to the conception or design of the work; final approval of the version to be published
YO Substantial contributions to the conception or design of the work; final approval of the version to be published
AB Substantial contributions to the conception or design of the work; final approval of the version to be published
MY Substantial contributions to the conception or design of the work; final approval of the version to be published
Article receive on Friday, February 23, 2018
 All scientific articles published at www.rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at www.rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()






 Read in English
Read in English
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket