![]()
![]()
Jinrong LiI; Tao ZhuI; Sufei YangI; Fan YangI; Jinhui WuI; Fei XiongI
DOI: 10.21470/1678-9741-2020-0592
ABSTRACT
A 32-month-old girl with patent ductus arteriosus, false tendon of left ventricle, mild pulmonary hypertension, and chronic cardiac insufficiency (cardiac function level I-II) was misdiagnosed with Marfan Syndrome and there was no improvement in her physical growth after operation for this disease. The preterm baby was finally diagnosed with Myhre Syndrome by clinical phenotypes and mutation of SMAD4 gene.
BMP = Bone morphogenetic protein
TGF-β = Transforming growth factor-β
INTRODUCTION
A 32-month-old girl was hospitalized because her growth and development were two years behind compared to same-age children. The patient was a twin (first pregnancy), and cesarean section was performed due to premature rupture of the mother’s membranes on 32 weeks of pregnancy. The birth weight of the patient was 1.4 kg, and her birth length was 34 cm. After preterm delivery, cardiac intervention and occlusion were performed when she was one year old because of patent ductus arteriosus, false tendon of left ventricle, mild pulmonary hypertension, and chronic cardiac insufficiency (cardiac function level I-II). But her physical growth was still retarded after the operation.
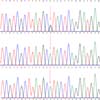
Physical examination of the child showed that the clinical phenotype was not consistent with the first genetic diagnosis of Marfan syndrome. Peripheral blood samples were collected from the proband and her parents and sister in August 2018 to perform gene sequencing. The clinical phenotypes of the patient in 2018 were patent ductus arteriosus, chronic cardiac insufficiency, severe malnutrition, and stunting. Taking clinical phenotypes and gene mutations together, it was found that there was a C > T (P.A1152A) mutation at C3455 point on chromosome 15 (OMIM:134797), which was predicted as variant of uncertain significance by the American College of Medical Genetics and Genomics. After the operation for heart structure improvement in the following year, the child still had serious growth and development disorders, language development retardation, hearing impairment, and autism. After defining and adding new clinical phenotypes, we found that the heterozygous variation of SMAD4 gene c.1498a > G (P.1500v) was more reasonable. Meanwhile, the mutation of SMAD4 at this point could lead to the abnormal expression of transforming growth factor beta (TGF-β), which was a strong pathogenic, consistent with previous report (Figure 1).

Discussion of Questions
Myhre syndrome is a rare disease that affects the connective tissue. SMAD4 is located in 18q21.2, and its gene mutation is the cause of Myhre syndrome. SMAD4 gene plays an important role in the process of cell chemical signal transduction. SMAD4 can achieve signal transduction by assisting the phosphorylation and oligomerization of TGF-β and bone morphogenetic protein (BMP) pathways, and its gene mutation affects the function of multiple organ systems. The mutation of SMAD4 gene can cause four different diseases, i.e., juvenile polyposis syndrome, hereditary hemorrhagic telangiectasia syndrome, Myhre syndrome, and pancreatic cancers, reflecting different clinical phenotypes caused by the same gene variation [1]. However, the Myhre syndrome caused by SMAD4 mutation has its own characteristics. The mutations all occur in the MH2 domain, which is necessary for SMAD4 oligomerization and TGF-β/BMP signal transduction. The restrictive pattern of SMAD4 mutation is the cause of the genetic homogeneity of Myhre syndrome, which is reflected in the clinical homogeneity [2,3]. Although Myhre syndrome has a variety of symptoms and signs that affect the body's multi-organ system, patients have similar clinical phenotypes, or even if some clinical symptoms are missing in the early stage, they will gradually become more obvious with aging [4] (Question A).
Congenital heart disease is a prominent problem in patients with Myhre syndrome. It is also an important basis for clinical judgment of factors affecting growth and development. Patients with Myhre syndrome often suffer from atrial septum, ventricular septal defect, patent ductus arteriosus, and valvular stenosis at birth, and they may also present with pulmonary artery stenosis and occlusion [5-7]. Heart problems may lead to poor growth. The child was born with patent ductus arteriosus, and gradually developed pulmonary hypertension and chronic cardiac insufficiency with aging. It was because of the serious heart problems that clinicians neglected the performance of other organ systems in the diagnosis of the disease, focused on the cardiovascular system in clinical practice, and got the wrong diagnosis (Question B).
In the process of gene examination, the same clinical phenotype may be caused by different gene mutations. In the analysis of a single prominent clinical phenotype, it is necessary to comprehensively summarize the clinical phenotype of the patient. When the result of gene mutation cannot explain the disease, we should carry out gene analysis from a new perspective. In this case, the gene data were analyzed for the first time only focusing on cardiovascular disease-related genes, thus making a clinical diagnosis of suspected Marfan syndrome. However, there was no catch-up growth after cardiac intervention, and the problem of growth retardation continued. At the same time, with aging, there was language retardation and autism-like behavior. Combined with the special facial features and bone and joint performance, we reinterpreted the results of gene exon sequencing, and finally detected the heterozygous variation of SMAD4 gene c.1498a > G (P.1500v) and corrected the clinical diagnosis (Question C).
BRIEF CONSIDERATION OF THE CASE REPORTED
The clinical manifestations of the syndrome are various, which may show different clinical characteristics with aging. The same clinical phenotype may be caused by different gene mutations, and the same gene mutation may also lead to completely different clinical manifestations. When conducting gene analysis, we must consider it comprehensively, rather than just focus on a single system.
LEARNING POINTS
The clinical phenotype is determined by the common factors of gene polymorphism and environment, and phenotypes of the same disease might be different at different ages.
The clinical phenotype is the basis of gene sequencing and interpretation, and the establishment of perfect genotype and clinical phenotype is an important method for the diagnosis of rare diseases.
Myhre syndrome is a multiple organ syndrome with multiple clinical manifestations.
Both gene variations of FBN1 and SMAD4 are easily misinterpreted as Marfan syndrome caused by FBN1 and misdiagnosed.
REFERENCES
1. Caputo V, Bocchinfuso G, Castori M, Traversa A, Pizzuti A, Stella L, et al. Novel SMAD4 mutation causing Myhre syndrome. Am J Med Genet A. 2014;164A(7):1835-40. doi:10.1002/ajmg.a.36544.
2. Picco P, Naselli A, Pala G, Marsciani A, Buoncompagni A, Martini A. Recurrent pericarditis in Myhre syndrome. Am J Med Genet A. 2013;161A(5):1164-6. doi:10.1002/ajmg.a.35892.
3. Genetic basis of Myhre syndrome. Bonekey Rep. 2012;1:26. doi:10.1038/bonekey.2012.29.
4. Nomura R, Miyai K, Nishimura G, Kashimada K, Morio T. Myhre syndrome: Age-dependent progressive phenotype. Pediatr Int. 2017;59(11):1205-6. doi:10.1111/ped.13413. [MedLine]
5. Alagia M, Cappuccio G, Pinelli M, Torella A, Brunetti-Pierri R, Simonelli F, et al. A child with Myhre syndrome presenting with corectopia and tetralogy of Fallot. Am J Med Genet A. 2018;176(2):426-30. doi:10.1002/ajmg.a.38560. [MedLine]
6. Lin AE, Michot C, Cormier-Daire V, L'Ecuyer TJ, Matherne GP, Barnes BH, et al. Gain-of-function mutations in SMAD4 cause a distinctive repertoire of cardiovascular phenotypes in patients with Myhre syndrome. Am J Med Genet A. 2016;170(10):2617-31. doi:10.1002/ajmg.a.37739.
7. Starr LJ, Grange DK, Delaney JW, Yetman AT, Hammel JM, Sanmann JN, et al. Myhre syndrome: clinical features and restric-tive cardiopulmonary complications. Am J Med Genet A. 2015;167A(12):2893-901. doi:10.1002/ajmg.a.37273.
Authors' roles & responsibilities
JL Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
TZ Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
SY Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
FY Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
JW Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
FX Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
Article receive on Friday, October 30, 2020
Article accepted on Monday, November 30, 2020
 All scientific articles published at www.rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at www.rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket