![]()
![]()
Herbert Coelho HortmannI; Homero Geraldo de OliveiraII; Renato Rocha RabelloIII; Eduardo Augusto Victor RochaIV; Sérgio Caporali de OliveiraV
DOI: 10.1590/S0102-76382010000200014
ABSTRACT
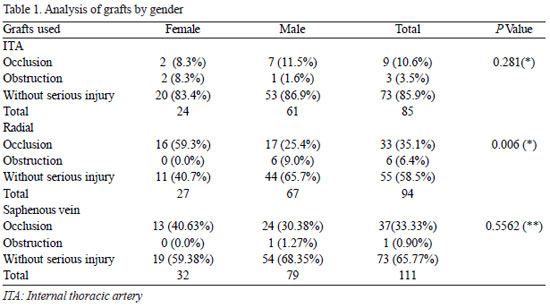
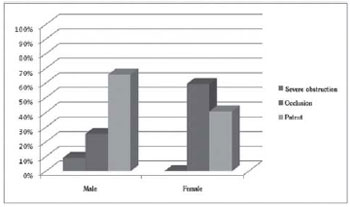
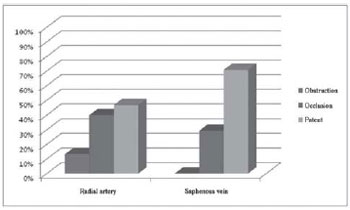
OBJECTIVE: To compare the radial artery and saphenous vein's patency in patients with recurrence of symptoms in a coronary artery bypass grafting (CABG). METHODS: Retrospective study. From January 1998 to December 2005, 469 CABGs were performed using the radial artery as a graft, in Vera Cruz Hospital in Belo Horizonte/ MG. Among the patients who underwent those surgeries, 94 presented ischemic changes in early or late postoperative period, which led them to be re-evaluated by coronary angiography. The grafts were divided in three groups: internal thoracic artery (ITA), radial artery (RA) and saphenous vein (SV), and they were stratified according to the severity of injury: uninjured or patent (< 70%), severe obstruction (70 to 99%) and occlusion. RESULTS: For the 94 patients in the study, 86 grafts of ITA, 94 of RA and 111 of SV were used. For the 86 ITA grafts, 73 (84.88%) were found patent. For the 94 RA grafts, 55 (58.51%) were found patent, and for the 111 SV grafts, 73 (65.76%) were uninjured. A statistically significant difference (P= 0.001) was found between RA and SV grafts, with a higher patency found for VS graft. For the RA grafts, women presented a worse result concerning the RA patency (65.7% and 40.7%), with P = 0.006. Concerning coronary revascularization, a statistically significant difference was found only for the grafts used for the right coronary, with a better result for the SV (P = 0.036). CONCLUSION: Radial artery (RA) presented worse results when compared to Saphenous vein (SV) as a second graft in a CABG, especially in women who were anastomosed in the right coronary artery.RESUMO
OBJETIVO: Comparar a perviedade da artéria radial e veia safena em pacientes com retorno dos sintomas após cirurgia de revascularização do miocárdio (CRVM). MÉTODOS: Estudo retrospectivo. No período de janeiro de 1998 a dezembro de 2005, foram realizadas 469 CRVMs com o uso da artéria radial dentre os enxertos, no Hospital Vera Cruz, em Belo Horizonte/MG. Destes, 94 pacientes apresentaram alterações isquêmicas no pós-operatório recente ou tardio e foram reestudados com cineangiocoronariografia. Os enxertos foram divididos em três grupos: artéria torácica interna (ATI), artéria radial (AR) e veia safena (VS), e foram estratificados segundo a gravidade das lesões: sem lesão grave (<70%), obstrução grave (70% a 99%) e oclusão. RESULTADOS: Nos 94 pacientes reestudados, foram utilizados 86 enxertos de ATI, 94 de AR e 111 de VS. Dos 86 enxertos de ATI, 73 (84,88%) se encontravam sem lesões graves; dos 94 enxertos de AR eram 55 (58,51%) e dos 111 enxertos de VS, 73 (65,76%) estavam livre de lesões graves. Houve diferença estatística (P= 0,001) entre os enxertos de AR e VS com maior perviedade da VS. As mulheres apresentaram pior resultado quanto à perviedade da AR (65,7% e 40,7%) com P= 0,006. Quanto à artéria coronária revascularizada, houve diferença entre os enxertos usados para artéria coronária direita, com melhor resultado da VS (P= 0,036). CONCLUSÃO: A AR mostrou-se com pior resultado que a VS como segundo enxerto na CRVM, principalmente em mulheres e quando anastomosada na coronária direita.

REFERENCES
1. Kirklin JW, Barratt-Boyes BG. Cardiac surgery. 3rd ed. New York:Churchill Livingstone;2003. p.354.
2. Loop FD, Lytle BW, Cosgrove DM, Stewart RW, Goormastic M, Williams GW, et al. Influence of the internal-mammaryartery graft on 10-year survival and other cardiac events. N Engl J Med. 1986;314(1):1-6. [MedLine]
3. Grondin CM, Campeau L, Lespérance J, Enjalbert M, Bourassa MG. Comparison of late changes in internal mammary artery and saphenous vein grafts in two consecutive series of patients 10 years after operation. Circulation. 1984;70(3 Pt 2): I208-12. [MedLine]
4. Lisboa LAF, Dallan LAO, Puig LB, Abreu Filho C, Leca RC, Dallan LAP, et al. Seguimento clínico a médio prazo com uso exclusivo de enxertos arteriais na revascularização completa do miocárdio em pacientes com doença coronária triarterial. Rev Bras Cir Cardiovasc. 2004;19(1):9-16. View article
5. Buffolo E, Maluf M, Barone B, Andrade JC, Gallucci C. Direct myocardial revascularization with the left gastro-epiploic artery. A new alternative to aortocoronary bypass. A case report. Arq Bras Cardiol. 1987;48(3):167-71. [MedLine]
6. Puig LB, Ciongolli W, Cividanes GV, Dontos A, Kopel L, Bittencourt D, et al. Inferior epigastric artery as a free graft for myocardial revascularization. J Thorac Cardiovasc Surg. 1990;99(2):251-5. [MedLine]
7. Borger MA, Cohen G, Buth KJ, Rao V, Bozinovski J, Liaghati-Nasseri N, et al. Multiple arterial grafts. Radial versus right internal thoracic arteries. Circulation. 1998;98(19 Suppl):II7-13.
8. Khot UN, Friedman DT, Pettersson G, Smedira NG, Li J, Ellis SG. Radial artery bypass grafts have an increased occurrence of angiographically severe stenosis and occlusion compared with left internal mammary arteries and saphenous vein grafts. Circulation. 2004;109(17):2086-91. [MedLine]
9. Locali RF, Buffolo E, Catani R. Artéria radial versus veia safena para revascularização do miocárdio: metanálise (não houve diferença estatisticamente significante). Rev Bras Cir Cardiovasc. 2006;21(3):255-61. View article
10. Possati G, Gaudino M, Prati F, Alessandrini F, Trani C, Glieca F, et al. Long-term results of the radial artery used for myocardial revascularization. Circulation. 2003;108(11):1350-4. [MedLine]
11. Modine T, Al-Ruzzeh S, Mazrani W, Azeem F, Bustami M, Ilsley C, et al. Use of radial artery graft reduces the morbidity of coronary artery bypass graft surgery in patients aged 65 years and older. Ann Thorac Surg. 2002;74(4):1144-7. [MedLine]
12. Acar C, Jebara VA, Portoghese M, Beyssen B, Pagny JY, Grare P, et al. Revival of the radial artery for coronary artery bypass grafting. Ann Thorac Surg. 1992;54(4):652-9.
13. Alves SF, Albuquerque DCM, Pelloso EA, Silveira WF, Labrunie A, Barros CR, et al. Avaliação angiográfica tardia do enxerto de artéria radial na cirurgia de revascularização do miocárdio. Rev Bras Cir Cardiovasc. 2003;18(1):32-9. View article
14. Buxton BF, Durairaj M, Hare DL, Gordon I, Moten S, Orford V, et al. Do angiographic results from symptom-directed studies reflect true graft patency? Ann Thorac Surg. 2005;80(3):896-900. [MedLine]
15. Achouh P, Boutekadjirt R, Toledano D, Hammoudi N, Pagny JY, Goube P, et al. Long-term (5- to 20-year) patency of the radial artery for coronary bypass grafting. J Thorac Cardiovasc Surg. 2009. [Epub ahead of print] [MedLine]
16. Lawton JS, Barner HB, Bailey MS, Guthrie TJ, Moazami N, Pasque MK, et al. Radial artery grafts in women: utilization and results. Ann Thorac Surg. 2005;80(2):559-63. [MedLine]
17. Hadinata IE, Hayward PA, Hare DL, Matalanis GS, Seevanayagam S, Rosalion A, et al. Choice of conduit for the right coronary system: 8-year analysis of Radial Artery Patency and Clinical Outcomes trial. Ann Thorac Surg. 2009;88(5):1404-9. [MedLine]
Article receive on Tuesday, December 22, 2009
 All scientific articles published at www.rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at www.rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket