![]()
![]()
Ikechukwu Andrew NwaforI; Aerra VickramIII; Kennedy O. OsenmoborIV
DOI: 10.21470/1678-9741-2020-0155
ABSTRACT
Introduction: In any country, the development and growth of open-heart surgery parallel stable political climate, economic growth, good leadership, and prudent fiscal management. These were lacking in Nigeria, which was under a military rule. The enthronement of democratic rule, in 1999, has caused desirable changes. The objective of this study is to report our experience with foreign cardiac teams that visited the National Cardiothoracic Center of Excellence, University of Nigeria Teaching Hospital, for seven years, in order to restart its open-heart surgery program.AML = Anterior mitral valve leaflet
AML = Atrial septal defect
AVCD = Atrioventricular canal defect
AVS = Aortic valve stenosis
CHD = Congenital heart disease
ECG = Electrocardiogram
ICU = Intensive care unit
LA = Left atrium
LSVC = Left superior vena cava
MAPCAS = Major aortic pulmonary artery collaterals
MVR = Mitral valve regurgitation
NCTCE = National Cardiothoracic Center of Excellence
NGOs = Nongovernmental organizations
OHS = Open-heart surgery
PA = Pulmonary artery
PAVD = Partial anomalous pulmonary venous drainage
PDA = Patent ductus arteriosus
PS = Pulmonary stenosis
RV = Right ventricle
SAHN = Save-A-Heart Nigeria
SAM = Subaortic membrane
TA = Truncus arteriosus
TETF = Tertiary Education Trust Fund
TOF = Tetralogy of Fallot
TVR = Tricuspid valve regurgitation
UNEC = University of Nigeria, Enugu campus
UNTH = University of Nigeria Teaching Hospital
VOOM = Vincent Ohaju Memorial
VSD = Ventricular septal defect
INTRODUCTION
The University of Nigeria Teaching Hospital (UNTH), in Ituku-Ozalla, Enugu, is the medical wing of the University of Nigeria Nsukka, or UNN, and it was established in 1970[1]. Four years later, in 1974, it became the first hospital in the country to carry out the first open-heart surgery (OHS) in Nigeria, with a foreign cardiac team led by a British-Egyptian, Sir Dr Yacoub, and an indigenous team led by late professor Fabian Udekwu[2]. As a result, the Federal Government of Nigeria, in 1978, designated UNTH, Enugu, a National Cardiothoracic Center of Excellence (NCTCE)[3].
Since that time, the center has been making efforts to establish itself as a leader in OHS, not only in Nigeria, but also in West Africa subregion[4]. However, the military rule coupled with its near total neglect of health system in the country led to the collapse of the center due to brain drain and inadequate facilities.
With the enthronement of democracy in Nigeria in 1999[5], efforts have been made to restart the open-heart program in the center. The options considered were staff training and equipment procurement. It was considered that the best way to achieve the desired training in an emerging country like ours was by receiving regular visits from foreign cardiac teams in the center who would perform OHS alongside the local team (cardiac mission model)[6,7]. This model has the advantage of treating the country’s patients at the same time. In addition, the model makes it possible for the visiting team to work in the usual environment of the local team. Moreover, the model makes for the improvement in the hospital’s infrastructure and equipment. Ideally, it ought to provide education, training, and sufficient experiences which eventually lead to full functional independent cardiac services that are sustainable over time[8].
Other options included sending the local team to established centers (e.g., India) for hands-on-training for a period not less than two years[9]. Furthermore, members of the local team may undergo abroad training on his or her own personal arrangement at different times and in different established centers. Training a complete cardiac team from a developing country is cumbersome, complex, and expensive[10]. In addition, to train a foreign resident in that setting is an added challenge[11].
The cardiac mission model, however, is not sustainable, as a lot of effort and expenditure are allocated towards surgery in few patients, led by experts who can afford short periods of stay away from their regular jobs[12]. Huge expenses are also incurred emanating from the air tickets of the team, procurement of visas, freight of needed equipment, and consumables including customs or excise duties at the airport or wharf. Accommodation and security of the visiting team are also an additional cost. Some foreign teams charge exorbitant fees, which are not affordable, and efforts are made to avoid high-risk cases, which would consume scarce resources, operating time, and tie down intensive care unit beds[13].
Efforts to establish a functional OHS program in Nigeria at other centers - like Lagos State University Teaching Hospital, or LASUTH, Ikeja, University College Hospital, or UCH, Ibadan, Lagos University Teaching Hospital, or LUTH, Idi-Araba, Gwagwalada Teaching Hospital, or GTH, Abuja, Obafemi Awolowo University Teaching Hospital, or OAUTH, Ile-If, Dr Joseph Nwiloh Cardiac Hospital, Adazi-ala, Anambra state, Ahmadu Bello University Teaching Hospital, or ABUTH, Zaria, and Orthan Dan Fodio University Teaching, or ODUTH, Sokoto state - have abysmally failed over the years because of emphasis on the surgical ‘safari’ method rather than on an educational program[9].
With return to democratic rule in 1999, efforts were made to restart the open-heart program at NCTCE, UNTH, Enugu. A purpose building, which was started in 1986, was completed and commissioned in 2001. The OHS program was going on. Unfortunately, the Enugu location had to be abandoned during moving to Ituku-Ozalla center, in 2007, which by then had no befitting arrangement for OHS. The Ituku-Ozalla center became ready for OHS in 2013.
METHODS
Different cardiac mission teams visited and treated patients for about 7.5 years (March, 2003 to October, 2019). A retrospective study was then carried out to compare surgical safari and educational program with a view to determine the levels of participation and competence of the local team, especially the surgeons. The data obtained from the hospital records database were the patients’ demographics, the number and type of cases managed, the number and frequency of visits of different cardiac mission teams, the level of participation and competence of a multidisciplinary local team, and funding of the program. The number of patients that had extracardiac surgery performed by the local and or foreign teams was excluded from the study.
Data were analyzed using IBM Corp. Released 2011, IBM SPSS Statistics for Windows, Version 20.0, Armonk, NY: IBM Corp. Rates and proportions were calculated with 95% confidence interval. The proportions were compared using Student’s t-tests. Level of significance was set at < 0.5.
RESULTS
During the study period, a total of 266 cardiac surgeries in 242 patients, involving both adults and children, were performed with a mean of 38 cases per year.
Table 1 displays the seven years of foreign cardiac mission in Nigeria with the number of patients; 33 mission trips were recorded, and 242 patients were treated.
| S/No. | Year | No. of missions | No. of patients treated | Percentages (%) |
|---|---|---|---|---|
| 1 | 2013 | 4 | 24 | 9.9 |
| 2 | 2014 | 3 | 17 | 7.0 |
| 3 | 2015 | 5 | 42 | 17.3 |
| 4 | 2016 | 5 | 53 | 21.9 |
| 5 | 2017 | 6 | 44 | 18.2 |
| 6 | 2018 | 5 | 40 | 16.5 |
| 7 | 2019 | 5 | 22 | 9.1 |
| Total | 33 | 242 | 100 |

Table 2 shows the distribution of the patients’ age ranges, including gender. The most affected were the age ranges of 1120 and 0-10 years. There were 112 females and 130 males.
| S/No. | Age ranges (years) | Females | Males | Total | Percentages (%) |
|---|---|---|---|---|---|
| 1 | 0-10 | 25 | 30 | 55 | 22.7 |
| 2 | 11-20 | 28 | 30 | 58 | 23.9 |
| 3 | 21-30 | 10 | 9 | 19 | 7.9 |
| 4 | 31-40 | 14 | 12 | 26 | 10.7 |
| 5 | 41-50 | 11 | 16 | 27 | 11.2 |
| 6 | 51-60 | 11 | 13 | 24 | 9.9 |
| 7 | 61-70 | 9 | 12 | 21 | 8.7 |
| 8 | 71-80 | 2 | 5 | 7 | 2.9 |
| 9 | 81-90 | 2 | 3 | 5 | 2.1 |
| Total | 112 (46.3%) | 130 (53.7%) | 242 | 100 |

Table 3 shows the distribution of adult cases managed. Heart valve surgery dominated, accounting for 108 (71.5%) cases, followed by coronary artery disease. A total of 151 cases were treated.
| S/No. | Types of adult cardiac cases | Number | Percentages (%) |
|---|---|---|---|
| 1 | Heart valves | 108 | 71.5 |
| 2 | Cardiac tumors (atrial myxoma) | 4 | 2.6 |
| 3 | Adult CHD | 20 | 17.4 |
| 4 | Coronary artery disease | 11 | 7.3 |
| 5 | Vegetations on the tricuspid | 1 | 0.7 |
| 6 | Endocarditis | 1 | 0.7 |
| 7 | Ascending aortic aneurysms | 6 | 3.9 |
| Total | 151 | 100 |

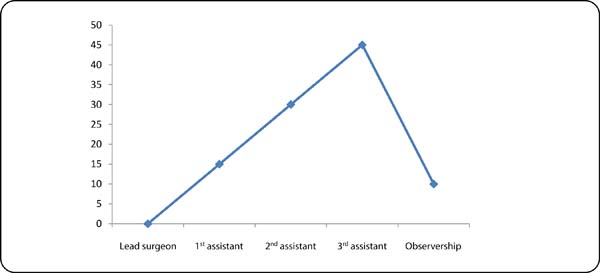
Figure 1 shows the level of participation of local surgeons. Throughout the period of seven years, no local surgeon ever led an OHS case. This partly accounts for the failure of the program because there was no sustainability.
Figure 2 shows the level of participation of local anesthetists. Throughout the period of seven years, less than 5% of local anesthetists led an OHS case. This partly accounts for the failure of the program because there was no sustainability.
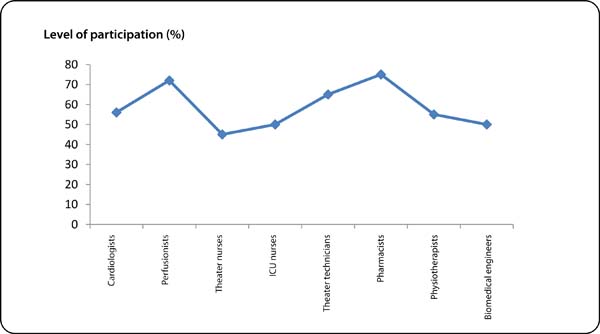
Figure 3 shows the level of participation of other members of local multidisciplinary cardiac team. Their participation was relatively better than those from anesthetists and surgeons. According to the hierarchy of training, there was no sustainability.
Table 4 shows the distribution of congenital heart diseases (CHD), both simple and complex types, treated. They are divided into isolated and combined lesions. Isolated tetralogy of Fallot (TOF) and ventricular septal defect (VSD) were dominant, representing 27.8% and 24.3% of the cases, respectively.
| S/No. | Types of pediatric cases treated | Number | Percentages (%) |
|---|---|---|---|
| 1 | TOF | 32 | 27.8 |
| 2 | VSD | 28 | 24.3 |
| 3 | ASD | 9 | 7.8 |
| 4 | MVR (rheumatic) | 2 | 1.7 |
| 5 | VSD +ASD | 3 | 2.6 |
| 6 | VSD + PDA | 11 | 9.5 |
| 7 | ASD + PAVD | 3 | 2.6 |
| 8 | PA + MAPCAS | 1 | 0.9 |
| 9 | AVCD | 5 | 4.3 |
| 10 | TA, type 1 | 3 | 2.3 |
| 11 | Severe TVR | 2 | 1.7 |
| 12 | VSD + SAM | 2 | 1.7 |
| 13 | Severe MVR + TVR + dilated LA | 1 | 0.9 |
| 14 | ASD + Cor-triatriatum | 1 | 0.9 |
| 15 | VSD + ASD + cor-triatriatum | 1 | 0.9 |
| 16 | VSD + ASD + AML | 1 | 0.9 |
| 17 | Common atrium + PDA | 1 | 0.9 |
| 18 | Large ASD + cor-triatriatum + valvular & supravalvular PS | 1 | 0.9 |
| 19 | VSD + ASD + SAM | 1 | 0.9 |
| 20 | ASD + PS | 2 | 1.7 |
| 21 | Severe PS + TVR + RV thrombus | 1 | 0.9 |
| 22 | SAM (AVS) + PDA | 3 | 2.6 |
| 23 | ASD + PS + LSVC | 1 | 0.9 |
| Total | 115 | 100 |
AML=anterior mitral valve leaflet; ASD=atrial septal defect; AVCD=atrioventricular canal defect; AVS=aortic valve stenosis; LA=left atrium; LSVC=left superior vena cava; MAPCAS=major aortic pulmonary artery collaterals; MVR=mitral valve regurgitation; PA=pulmonary artery; PAVD=partial anomalous pulmonary venous drainage; PDA=patent ductus arteriosus; PS=pulmonary stenosis; RV=right ventricle; SAM=subaortic membrane; TA=truncus arteriosus; TOF=tetralogy of Fallot; TVR=tricuspid valve regurgitation; VSD=ventricular septal defect

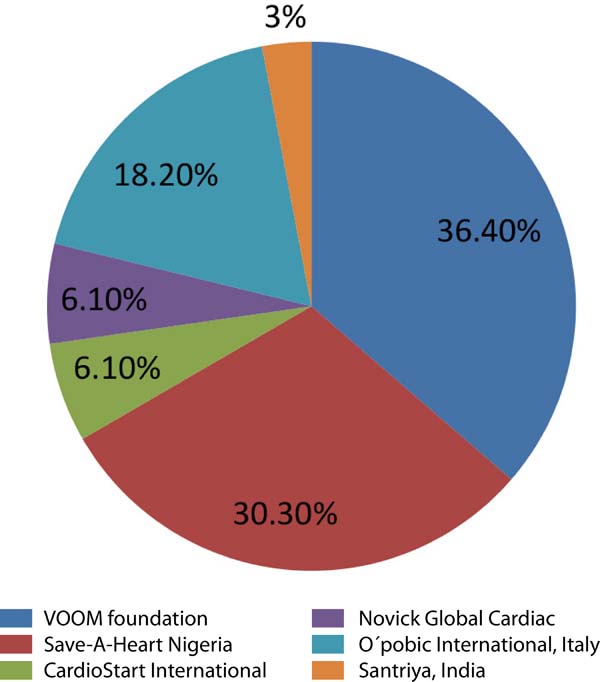
Figure 4 shows the distribution of the foreign cardiac teams that visited and operated on patients under mission model. Here the two nongovernmental organizations (NGOs) (Vincent Ohaju Memorial [VOOM] and Save-A-Heart Nigeria [SAHN]), both led by Nigerians in Diaspora, dominated. Both emphasized on surgical safari and this accounted for the failure of the program after seven years.
Tables 5 and 6 shows the distribution of sources of fund for the OHS program and methods of fund utilization. Here, the Tertiary Education Trust Fund (TETF) constituted the major share. However, after seven years of mission model, most of the equipment have spoilt without replacement. This also accounts for why the program is not sustainable. Closely following TETF from the Federal Government of Nigeria through the National Universities Commission, or NUC, are the Federal Ministry of Health and the UNTH management for their varied roles, as displayed in the tables.
| S/No. | Sources of fund | Description of fund utilization | Remarks |
|---|---|---|---|
| 1 | Tertiary Education Trust Fund | Medical equipment | 40% (see Table 6) |
| 2 | Federal Ministry of Health | Payment of salaries of local multidisciplinary cardiac team | 20% |
| 3 | UNTH management | Air tickets, visas, accommodation, transportation, feeding and security of visitors, consumables, generator (power supply), excise duties of donated equipment | 20% |
| 4 | Foreign donations (foreign missions) | Used equipment, consumables, honorarium, air tickets | 8% |
| 5 | Rotary Club | Payment of surgical fees | 2% |
| 6 | Patients and relatives | Payment of surgical fees, blood donations | 2% |
| 7 | Bigaard Seminary School Enugu (seminarians), medical students (UNEC) | Blood donations | 1.5% |
| 8 | Public-spirited individuals | Payment of surgical fees and blood donations | 1.5% |
| 9 | Enugu state government | Payment of surgery fees for pediatric cases | 5% |

DISCUSSION
OHS is a type of surgery that requires an exposure of the internal structure of the heart. This often requires cardiopulmonary bypass. Due to the functions of the heart, this procedure requires highly skilled manpower, sophisticated equipment, and infrastructure[14]. These essentials are lacking in many countries in sub-Saharan African countries, except South Africa, Egypt, and Sudan. In many West African countries, heart surgery started with closed heart procedure (mitral commissurotomy, repair of patent ductus arteriosus [PDA], pericardiectomy, etc) by trained cardiothoracic surgeons from the United Kingdom, United States of America, and France, as early as 1960[13]. However, countries like Ghana, Nigeria, and Côte d’Ivoire began to perform OHS with aid of foreign cardiac teams[15]. This momentum was sustained through the 1980s before most of the programs failed due to economic challenge, occasioned by military rule and civil strife, including interprofessional conflicts[16].
In Nigeria, a foreign cardiac team with the local multidisciplinary cardiac team performed the first OHS in our institution. This singular effort, in addition to many others, endeared the institution to the Federal Government of Nigeria. Consequently, the local personnel and equipment, including the infrastructure that carried the first OHS, were by executive order of the Federal Government of Nigeria proclaimed a NCTCE in 1984[3]. Shortly afterwards, the center’s activities dwindled due to military rule, corruption, and brain drain. Between 1974 and 2000, about 102 cases of OHS were carried out[6].
With return to democratic rule in 1999, efforts were made to revitalize the center by continuation of the foreign cardiac mission model, using Nigerians in Diaspora as anchors. The first mission in a democratic set-up was by the International Heart Foundation, or ICF, in partnership with Kanu Heart Foundation, or KHF, precisely in 2003[17]. Ten years later, other cardiac missions started and became relatively regular (Table 1 and Figure 4).
During these periods, about 266 cases have been treated over seven years, averaging 38 cases per year; 130 (53.7%) males and 112 (46.3%) females, both adults and children, were involved (Table 2). Male to female ratio was 1.0:0.9. In these series, heart valve diseases (71.5%), followed by adult CHD (17.4%), were the commonest indications for intracardiac surgery in adult patients (Table 3). In the pediatric group, isolated TOF (n=32, 27.8%) and isolated VSD (n=28, 24.3%) followed by VSD and PDA (n=11, 9.5%) were the commonest indications for OHS (Table 4). For the first time, complex types of CHD were successfully managed[18]. They were truncus arteriosus type 1[19] and congenital tricuspid valve disease (congenital absence of both anterior and posterior leaflets), as well as pulmonary atresia with major aortic pulmonary artery collaterals (Table 4). Greater percentages of patients with mitral and aortic valve diseases had prosthetic replacement in view of the fact that they were predominantly rheumatic and also that the chances of having a second surgery would be difficult financially.
The age of the patients operated on ranged from five months to 86 years, with a mean of 43.2 years. The age range of patients mostly involved in the OHS procedure was 11-20 years (n=58, 23.9%), followed by 0-10 years (n=55, 22.7%). The least affected age ranges were 71-80 and 81-90 years (n=7, 2.9% and n=5, 2.1%, respectively) (Table 2).
Despite the reasonable number of cases performed, the participation of the local surgeons and anesthetists was very low (Figures 1 and 2). These are the highest skilled professionals in the hierarchy of a cardiac team based on their training. In this model, that lasted a week or two (each visit) with irregular frequency, training of the surgeons or the anesthetists was highly inadequate. The different foreign surgeons were often uncomfortable allowing a local surgeon to lead an OHS case. Also, some Nigerians in Diaspora running the NGOs (VOOM and SAHN) saw the mission model as a surgical safari rather than an educational program (Figure 3). To this end, they did not see the long-term benefit of a local team taking over the performance of the OHS program.
Therefore, emphasis was that a cardiac surgeon and or anesthetist should undergo proper hands-on-training in reputable centers abroad with high volume of surgeries in a year[9]. The European Association of Cardiothoracic Surgeons and its International Committee do not believe that the best solution in achieving a sustainable cardiac program in a developing country is by sending a foreign cardiac team there[20]. However, in a similar study by Velebit et al.[7], a team of fully trained specialists did a cardiac mission in Tbilisi, Georgia, for a period of five years where the frequency was monthly, with one-week duration, and with an average of 10 times in a year. After five years, the local team was able to become independent and had performed 181 cases out of 204, within the first seven months in 2008, while the remaining was done by a foreign team during irregular support visits related to difficult cases[7].
In Nigeria, with a population of 200 million people[21] and with supposedly six government centers, ours inclusive, trying to perform an OHS through mission model was far from ideal. The ideal would have been the government supporting one or two centers to become proficient. It is these proficient centers that ultimately will drive the local growth of skills in OHS nationally. Other middle skilled members of the local team were easily taught, and their level of participation was high (Figure 3).
From the onset, three modalities were considered in revitalizing the OHS program in our center. The cheapest of them was the mission model. In low-income countries like Nigeria, with double burden of diseases (communicable and noncommunicable), getting a near ideal cardiac center requires huge investments in procuring high-tech equipment, building infrastructure, and training personnel. Indeed, it would not have been possible without aids from the Nigerian government, Nigerians in Diaspora, public-spirited individuals, and foreign donations (Table 5). Most of the countries in the sub-region are very poor and in a study by Edwin et al.[22], it was shown that no existing cardiac center in the sub-region came into being without government interventions[23]. Thus, as pointed out by Dearani et al.[24], humanitarian outreach activities should focus on education and sustainability and surgical tourism should be limited to those centers that will never have the capacity to have a free-standing cardiothoracic program[22]. Evidently, it was documented that success of cardiac mission should not be measured by the number of successful operations of any given mission, but by the successful operations the local team were able to perform after the departure of the visitors[24,25]. In our own situation, we had 33 mission trips and carried out about 266 cardiac procedures in 242 patients over a seven-year period, yet the locals had not transited to independence even for minor cases like atrial septal defect, VSD, and minor forms of TOF, as well as valves in adults (Table 1). The main goal of the mission should be to provide teaching to local staff and implement methods and techniques to support the improvements in the care of patients in the long run[22].
CONCLUSION
The adoption of a cardiac mission model to revitalize the OHS program following the enthronement of democratic rule in our country as well as helping indigent patients with both congenital and acquired heart diseases and creating awareness was good. But this surgical safari was not sustainable. However, this method is like giving someone a fish any time he demanded it. The best way was to have incorporated teaching the person how to fish, i.e., equipping and developing the local team for sustainability.
REFERENCES
1. Okaro JM, Umezulike AC, Onah HE, Chukwuali LI, Ezugwu OF, Nweke PC. Maternal mortality at the university of Nigeria teaching hospital, Enugu, before and after Kenya. Afr J Reprod Health. 2001;5(2):90-7. doi:10.2307/3583434.
2. Edwin F, Frimpong-Boateng K. Open-heart surgery and coronary artery bypass grafting in Western Africa. Pan Afr Med J. 2011;9:3. doi:10.4314/pamj.v9i1.71175.
3. Anyanwu CH, Iheanacho H, Okoro E, et al. Initial experience with open heart surgery in Nigeria. Trop Cardiol. 1982;8:123-127.
4. Eze JC, Ezemba N. Open-heart surgery in Nigeria: indications and challenges. Tex Heart Inst J. 2007;34(1):8-10. [MedLine]
5. Ogundiya IS. Democracy and good governance: Nigerias’ dilemma. Afr J Pol Sci Int Relat. 2010;4(6):201-8.
6. Gosh P. Setting up Open Heart Surgery in a developing country: Asian Cardiovasc Thorac Ann. 2005;13(4):299-301. [MedLine]
7. Velebit V, Montessuit M, Bednarkiewicz M, Khatchatourian G, Mueller X, Neidhart P. The development of cardiac surgery in an emerging country: a completed project. Tex Heart Inst J. 2008;35(3):301-6.
8. Novick WM, Molloy F, Bowtell K, Forsberg B, Pavanic M, Polivenok I, et al. Pediatric cardiac service development programs for low- and middleincome countries in need of improving or initiating local services. Front Pediatr. 2019;7:359. doi:10.3389/fped.2019.00359.
9. Nwafor IA, Eze JC, Nwafor MN; National Cardiothoracic Center of Excellence (NCTCE), University of Nigeria Teaching Hospital (UNTH), Ituku-Ozalla, Enugu, Nigeria. Establishing a sustainable open heart surgery programme in Nigeria, a low-income country: which is the best model? Cardiol Young. 2019;29(12):1489-93. doi:10.1017/S1047951119002531. [MedLine]
10. Isaacson G, Drum ET, Cohen MS. Surgical missions to developing countries: Ethical conflicts. Otolaryngol Head Neck Surg. 2010;143(4):476-9. doi:10.1016/j.otohns.2010.05.011.
11. Yacoub MH. Establishing pediatric cardiovascular services in the developing world: a wake-up call. Circulation. 2007;116(17):1876-8. doi:10.1161/CIRCULATIONAHA.107.726265.
12. Stolf NA. Congenital heart surgery in a developing country: a few men for a great challenge. Circulation. 2007;116(17):1874-5. doi:10.1161/CIRCULATIONAHA.107.738021.
13. Nwiloh JO, Mobolaji AO, Adebola PA. Heart surgery practice in sub-Saharan Africa: single Nigerian institutional midterm results and challenges. W J Cardiovasc Sur. 2014;4(3):35-41. doi: 10.4236/wjcs.2014.43006.
14. Gleen W G. Surgery and Healing in the Developing world, Georgetown (TX): Landes Bioscience; 2005. 485 p.
15. Oludara MA, Nwiloh J, Fabamwo A, Adebola P. Commencing open heart surgery in resource limited countries: lessons from the LASUTH experience. Pan Afr Med J. 2014;19:105. doi:10.11604/pamj.2014.19.105.4848.
16. Coulibaly AO, Ouattara K, Kangah KM, Yangni-Angate H, Tanauh Y, Longechaud A, et al. . Chirurgie. 1987;113(5):470-5. French.
17. Orjiako AB. Interprofessional conflict resolution in the health sector. Niger J Med. 1996;5:28-31.
18. The Kanu Heart Foundation . Nigeria: KANU; c2020 . Available from:
19. Nwafor IA, Chinawa JM, Adiele DK, Arodiwe IO, Ezemba N, Eze JC, et al. Management of complex CHD at the national cardiothoracic center of excellence, university of Nigeria teaching hospital, Enugu: the role of foreign cardiac missions in 3.5 years. Cardiol Young. 2017;27(6):1174-9. doi:10.1017/S1047951116002766. [MedLine]
20. Nwafor IA, Novick W, Adiele DK, Eze JC, Ezemba N, Chinawa JM, et al. Repair of truncus arteriosus, type 1 in Nigeria. a case report. J Vasc Med Surg. 2016;4:264. doi:10.4172/2329-6925.1000264.
21. Roques F, Nashef SA, Michel P, Gauducheau E, de Vincentiis C, Baudet E, et al. Risk factors and outcome in European cardiac surgery: analysis of the EuroSCORE multinational database of 19030 patients. Eur J Cardiothorac Surg. 1999;15(6):816-22; discussion 822-3. doi:10.1016/s1010-7940(99)00106-2.
22. Edwin F, Tettey M, Aniteye E, Tamatey M, Sereboe L, Entsua-Mensah K, et al. The development of cardiac surgery in West Africa--the case of Ghana. Pan Afr Med J. 2011;9:15. doi:10.4314/pamj.v9i1.71190.
23. Akinyemi A, Isiugo-Abanihie UC. Demographics dynamics and development in Nigeria: issues and perspective. 2014;27(2 Supp):239-48. doi:10.11564/27-2-471.
24. Dearani JA, Jacobs JP, Bolman RM 3rd, Swain JD, Vricella LA, Weinstein S, et al. Humanitarian outreach in cardiothoracic surgery: from setup to sustainability. Ann Thorac Surg. 2016;102(3):1004-11. doi:10.1016/j.athoracsur.2016.03.062. [MedLine]
25. Nina VJDS, Farkas EA, Nina RVAH, Marath A. Humanitarian missions: a call for action and impact from cardiovascular surgeons. Braz J Cardiovasc Surg. 2017;32(6):III-V. doi:10.21470/1678-9741-2017-0197.
Authors' roles & responsibilities
IAN Substantial contributions to the design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
AV Drafting the work or revising it critically for important intellectual content
KOO Substantial contributions to the design of the work; or the acquisition, analysis, or interpretation of data for the work; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; final approval of the version to be published
Article receive on Wednesday, April 8, 2020
Article accepted on Thursday, April 9, 2020
 All scientific articles published at www.rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at www.rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()





 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket