![]()
![]()
Margarete Diprat TrevisanI; Diene Gomes Colvara LopesII; Renato Gorga Bandeira de MelloIII; Fabrício Edler MacagnanIV; Adriana KesslerV
DOI: 10.5935/1678-9741.20150085
ABSTRACT
OBJECTIVE: To compare the efficacy of a cycle ergometer-based exercise program to a standard protocol on the increment of the maximum distance walked during the six-minute walk test in the postoperative rehabilitation of patients submitted to coronary artery bypass grafting.
METHODS: A controlled clinical trial pilot, blinded to the outcome, enrolled subjects who underwent coronary artery bypass grafting in a hospital from Southern Brazil. Subjects were designated for the standard physical rehabilitation protocol or to an alternative cycle ergometer-based protocol through simple random sampling. The primary outcome was the difference in the maximum distance walked in the six-minute walk test before and after the allocated intervention.
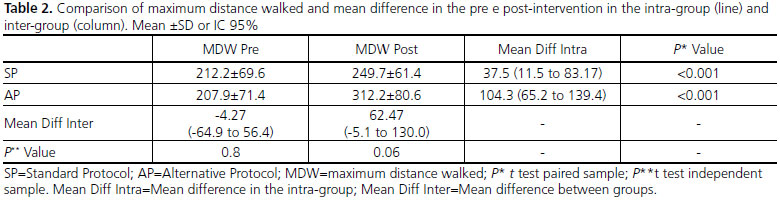
RESULTS: Twenty-four patients were included in the analysis, 10 in the standard protocol and 14 in the alternative protocol group. There was an increment in the maximum distance walked in both groups, and borderline superiority in the intervention group comparing to the control group (312.2 vs. 249.7; P=0.06).
CONCLUSION: There was an increase in the maximum distance walked in the alternative protocol compared to the standard protocol. Thus, it is postulated that the use of a cycle ergometer can be included in physical rehabilitation in the hospital phase of postoperative coronary artery bypass grafting. However, randomized studies with larger sample size should be conducted to assess the significance of these findings.
6MWT = Six-minute walk test
ACSM = American College of Sports Medicine
AMI = Acute myocardial infarction
AP = Alternative protocol
BMI = Body mass index
BP = Blood pressure
BPM = Beats per minute
CABG = Coronary artery bypass grafting
CAD = Coronary artery disease
CPMR = Cardiopulmonary and metabolic rehabilitation programs
ECG = Electrocardiogram
HR = Heart rate
MDW = Maximum distance walked
PUCRS = Pontifical Catholic University of Rio Grande do Sul
SP = Standard Protocol
SPSS = Statistical Package for the Social Sciences
WHO = World Health Organization
INTRODUCTION
Coronary artery disease (CAD) is a major cause of death worldwide[1]. The World Health Organization (WHO) estimates that in addition to being the leading cause of death, cardiovascular disease is also cause of disability, loss of productive capacity and quality of life[2-4].
Coronary artery bypass grafting (CABG) is performed as an effective treatment option in different scenarios of CAD[5] and aims to improve survival, prevent acute myocardial infarction (AMI), reinfarction, improve ventricular function and relieve anginal symptoms[6-9].
Despite its effectiveness, CABG is a highly invasive procedure, often associated with long time of bed rest, reduced cardiorespiratory capacity, loss of strength and muscle mass, as well as physical deconditioning[10,11]. To minimize such deleterious effects, cardiopulmonary and metabolic rehabilitation programs (CPMR) are crucial in the recovery process and must be started as soon as possible[12].
Physical rehabilitation protocols often include ambulation and gait training. However, it is difficult to be conducted in the daily practice due to patient's physical limitations, increased risk of falls and insecurity from the patient and the professional who apply the protocol[13,14]. Additionally, it is harder to monitor vital signs, such as the blood pressure surveillance, and as well as the exercise intensity, especially when walk training programs are applied in corridors and stairways.
In this scenario, the cycle ergometer becomes a possible alternative. It is a training equipment, already used in rehabilitation programs after AMI, that allows to monitor heart rate (HR), blood pressure (BP) and even cardiac electrical activity through electrocardiogram (ECG). Such parameters are extremely important in the first phase of CPMR programs[2,3,15,16]. Moreover, the cycle ergometer rehabilitation program can be applied even in patients with physical limitations due to orthopedic and/or neurological diseases[3,17].
Thus, the objective of this study was to compare the efficacy of an alternative exercise program using a cycle ergometer to a standard rehabilitation protocol during the CPMR phase I, in the postoperative period of CABG, on the maximum distance walked assessed by the six-minute walk test (6MWT).
METHODS
Design and study population
It is a pilot controlled clinical trial study, investigator-blinded to the outcome. The individuals included were aged 50 or older of both genders who underwent CABG at the São Lucas Hospital, from the Pontifical Catholic University of Rio Grande do Sul (PUCRS), between December 2011 and October 2012. The allocation to treatment was performed through a simple random sampling, drawing to the treatment group the first individual included and respecting the allocation to groups in alternating sequence.
Individuals with physical limitations (orthopedic and/or neurological disorders) or who had complications in the perioperative or postoperative period (bleeding requiring reoperation, sepsis, mediastinitis, prolonged mechanical ventilation (>24 hours), reintubation, cerebrovascular accident, AMI, pulmonary embolism, acute renal failure, unstable angina or malignant arrhythmias) were excluded.
Description of variables
Sociodemographic variables such as gender, age and smoking history were collected through a questionnaire standardized for the study. Anthropometric measurements (weight in kg and height in meters), variables related to the surgery and clinical conditions in the postoperative period were collected by review of pre and postoperative evaluation available in the patient record.
The 6MWT test was conducted by a physical therapist blinded to the intervention according to the American Thoracic Society protocol[18]. The test was conducted in a level corridor 30 meters long with markings every 2.5 meters. Participants were oriented to walk as long as possible during six minutes and were not allowed to run during the test. HR (beats per minute - bpm), and peripheral oxygen saturation (SpO2 -%), were observed by pulse oximetry before and after the 6MWT. In addition, blood pressure (mmHg) and rate of perceived exertion, using the Borg's perceived exertion scale, were also measured. The Borg's scale rates from zero to ten the perception of fatigue due to effort. After the 3rd minute (during the test) and at the end of the 6th minute, HR, SpO2 and Borg were recorded. For the 6MWT execution, the evaluator was standing immediately by the patient's side, guiding and encouraging the participant to walk as fast as possible. The 6MWT was performed on the 3rd postoperative day and repeated on the 6th day after CABG. During the test, any sign and symptom resulting from physical exertion were recorded. The outcome chosen for the 6MWT was the maximum distance continuously walked for both intra and inter-group comparison.
Intervention
Control - Standard Protocol (SP)
Patients in this group had physical therapy conducted by the hospital staff and the standard rehabilition protocol was performed. In this protocol, on the 3rd postoperative day, position in bed was conducted as well as chest clearance maneuvers and bronchial hygiene when needed. Pulmonary re-expansion maneuvers, specific physical exercises (if indicated) and ambulation were performed in the hospital room. In the 4th to the 7th postoperative day, the same treatment was executed, except ambulation which was made in the hospital corridor. From the 5th postoperative day, participants had to climb and descend stairs with supervision. The average duration of the standard physical therapy protocol was 20 minutes and it was performed primarily during the morning and also in the afternoon.
Alternative Protocol (AP) - Cycle Ergometer
In this group, physical therapy techniques conducted with the participants were similar to the standard group, except for the substitution of walking and stairs exercises to cycle ergometer exercise, since the 3rd postoperative day. Participants performed 20 minutes of exercise on a cycle ergometer during the morning and another 20 minutes in the afternoon. HR (calculated as recommended by the American College of Sports Medicine (ACSM) and tolerated up to 30 bpm above the resting HR), BP, SpO2 and rate of perceived exertion through the Borg Scale, as described previously, were monitored during cycling. The cycle ergometer training was monitored by trained researchers.
Cycling was interrupted in the presence of signs and symptoms of effort intolerance. The goal was to keep 20 minutes steadily, but depending on the participant physical conditions, the first sessions were intermittently held.
Protocol Operationalization and Implementation
Participants' identification started from checking the scale of heart surgery at the hospital on the day of discharge from the postoperative care of heart surgery, which usually happened on the 3rd day after CABG. At this moment, the medical team responsible to the patient contacted the physical therapist researcher, allowing the patient's participation in the research. Then, patients were informed about the protocol and after signing the informed consent, the initial data collection was conducted, which consisted of a questionnaire containing participants sociodemographic data and their clinical characteristics. In both groups, the 6MWT was performed on the 3rd postoperative day and repeated on the day of discharge or on the 6th postoperative day. The CPMR program also began on the 3rd postoperative day with the last training happening between the 4th and the 5th session (depending on the day of discharge) and consisted of two sessions daily, one in the morning and another in the afternoon.
Statistical Analysis and Sample Calculation
To detect a statistically significant difference of 50 meters between the mean maximum distance walked in the 6MWT in two-tailed test with 80% power and possibility of type I error below 5%, it was calculated a sample size of 12 subjects to be included in each group.
The data collected were entered into a Microsoft Excel® spreadsheet. Categorical variables were reported in percentage, and continuous variables as means and standard deviation. Variables were tested for distribution using the Shapiro-Wilk test. Distribution of all variables tested, in both groups, was normal. Thus, the comparison between the distance walked before and after intervention in each group was performed by the t test for paired samples and the comparison between groups was also done by the t test for independent samples. Comparison of categorical variables was performed using the chi-square test. For analyzes the Statistical Package for the Social Sciences (SPSS® for Windows® version 16 - USA) was used.
Ethical Considerations
The research project was reviewed and approved by the Medical School Scientific Committee and PUCRS Research and Ethics Committee (registration number 09/04813). All participants consented to participate after the presentation and explanation of terms included in the Informed Consent.
RESULTS
Twenty-seven participants who underwent CABG were included in this study. However, two patients were excluded due to early hospital discharge (less than three rehabilitation sessions) and another one was excluded by clinical decompensation. Thus, ten participants were included in the analysis in the SP group and 14 in the AP group.
As described in Table 1, the sample consisted predominantly of men, mean age around 60 years old. Comparison of the maximum distance walked (MDW) in the 6MWT, pre- and post-intervention in each group and between the groups, is presented in Table 2. There was an increment in the MDW post-intervention in both groups with a tendency to be longer in the AP group compared the SP group (312.2±80.6 vs. 249.7±61.4 m; P=0.06).

There was no statistically significant difference between groups when comparing HR, SpO2 and the Borg's scale means in the post-intervention period.
DISCUSSION
This study demonstrated that there was a similar increase in the MDW in both groups after implementation of rehabilitation protocols after CABG. However, there was a trend for superiority of the alternative protocol, which used a cycle ergometer to replace walking and stair exercises. Furthermore, the cycle ergometer protocol allowed participants to be monitored continuously for cardiorespiratory variables during the rehabilitation program, favoring a better control of exercise intensity.
It has been demonstrated, previously, that the distance walked during the 6MWT varies according to body mass index (BMI)[19], being smaller in those individuals with grater BMI values, result also showed in this present study which found that individuals with BMI < 25 kg/m2 walked more than those with a BMI> 25 kg/m2 (565.45±101.56m vs. 457.35±92.18m). However, even that the average BMI was greater in the alternative protocol compared to the standard one, there was a trend of superiority achieved in the MDW post-rehabilitation using the cycle ergometer. Moreover, in the cycle ergometer protocol, MDW was shorter than in the SP, suggesting a lower initial physical capacity in the AP. Even with these factors, in this study, there was a tendency of improvement in the MDW post-intervention in the cycle ergometer group, suggesting a conservative bias to the results. These findings propose the possibility of even greater benefits using the cycle ergometer in improving functional performance of these individuals compared to the SP.
Because this was an exploratory intervention not applied in a similar population yet, there is no evidence available for direct comparison. However, a study with hypertensive patients measured and compared the behavior of acute BP, HR and perceived exertion during a circuit of resistance exercise versus submaximal aerobic exercise using a cycle ergometer. The authors found that participants allocated to the cycle ergometer group had a smaller increase in HR, systolic blood pressure and perceived exertion, suggesting that the use of a cycle ergometer offers safer responses to cardiac patients[20].
The goal of proposing an alternative rehabilitation protocol using a cycle ergometer is to avoid the deleterious effects of prolonged bed rest safely from the cardiorespiratory view. An important advantage of this type of physical activity is an effective increase in systemic circulation without excessive burdens on the cardiopulmonary system, since muscle contraction is predominantly dynamic, when no resistance to the pedal is added. Other advantages justify the use of this ergometer: a potential reduction in the risk of falls, the possibility of performing a constant and more lasting effort and the possibility of monitoring vital signs at the metabolic demand peak caused by exercise[16,21].
Additionally, studies have shown that the early use of a cycle ergometer in intensive care unit patients, even during ventilation, increases muscle strength, also improving functional capacity, with similar cardiovascular benefits achieved in treadmill rehabilitation[22,23]. Adding to the effectiveness of the method, an important advantage is that the interruption of effort occurs in a safer way, since the patient is already seated and supported with both hands. Therefore, even if the interruption happens in an unexpected and abrupt way, the physical therapist will be in a better position to handle the situation and ask for support when needed. Another relevant point is the ease in having oxygen support, if needed, even during the protocol implementation.
Some limitations of this study must be highlighted: (1) limited sample size, reflecting reduced power to identify the significant differences; (2) simple random sampling, in alternately sequence, which can enable the occurrence of heterogeneity among groups. However, this is a new protocol, evaluated in a pilot study. As a result, the power to identify differences between groups is limited and there was uneven distribution of possible confounding variables between the control and alternative groups. Nevertheless, the differences are possibly associated with a conservative bias, as longer MDW in the 6MWT pre-intervention and lower BMI were found in the control group.
CONCLUSION
This study demonstrated that both protocols were similarly effective in promoting increased MDW in the 6MWT in patients who underwent physical therapy rehabilitation after CABG, with a tendency of superiority in the cicloergometer group. However, a phase III randomized clinical trial is needed to evaluate the significance of these reported findings.
REFERENCES
1. Ramos GC. Aspectos relevantes da doença arterial coronariana em candidatos à cirurgia não cardíaca. Rev Bras Anestesiol. 2010;60(6):662-5.
2. Mackay J, Mensah G. Atlas of heart disease and stroke. Geneva: WHO; 2004.
3. Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE Jr, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50(7):e1-e157. [MedLine]
4. Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1999 guidelines for the management of patients with acute myocardial infarction). J Am Coll Cardiol. 2004;44(3):671-719. [MedLine]
5. Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG, et al. 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124(23):e652-e735. [MedLine]
6. Botega FS, Cipriano Júnior G, Lima FVSO, Arena R, Fonseca JHP, Gerola LR. Cardiovascular behavior during rehabilitation after coronary artery bypass grafting. Rev Bras Cir Cardiovasc. 2010;25(4):527-33. [MedLine] View article
7. Nery RM, Martini MR, Vidor CR, Mahmud MI, Zanini M, Loureiro A, et al. Alterações na capacidade funcional de pacientes após dois anos da cirurgia de revascularização do miocárdio. Rev Bras Cir Cardiovasc. 2010;25(2):224-8. [MedLine] View article
8. Iglézias JCR, Chi A, Talans A, Dallan LAO, Lourenção Júnior A, Stolf NAG. Desfechos clínicos pós-revascularização do miocárdio no paciente idoso. Rev Bras Cir Cardiovasc. 2010;25(2):229-33. [MedLine] View article
9. Cantero MA, Almeida RMS, Galhardo R. Análise dos resultados imediatos da cirurgia de revascularização do miocárdio com e sem circulação extracorpórea. Rev Bras Cir Cardiovasc. 2012;27(1):38-44. [MedLine] View article
10. Guizilini S, Gomes WJ, Faresin SM, Carvalho ACC, Jaramillo JI, Alves FA, et al. Efeitos do local de inserção do dreno pleural na função pulmonar no pós-operatório de cirurgia de revascularização do miocárdio. Rev Bras Cir Cardiovasc. 2004;19(1):47-54. View article
11. Baptista VC, Palhares LC, Oliveira PPM, Silveira Filho LM, Vilarinho KAS, Severino ESBO, et al. Teste de caminhada de seis minutos como ferramenta para avaliar a qualidade de vida em pacientes submetidos à cirurgia de revascularização miocárdica. Rev Bras Cir Cardiovasc. 2012;27(2):231-9. [MedLine] View article
12. Fletcher GF, Balady GJ, Amsterdam EA, Chaitman B, Eckel R, Fleg J, et al. Exercise standards for testing and training: a statement for healthcare professionals from the American Heart Association. Circulation. 2001;104(14):1694-740. [MedLine]
13. Titoto L, Sansão MS, Marino LHC, Lamari NM. Reabilitação de pacientes submetidos à cirurgia de revascularização do miocárdio: atualização da literatura nacional. Arq Ciênc Saúde. 2005;12(4):216-9.
14. Regenga MM. Fisioterapia em cardiologia: da UTI à reabilitação. São Paulo: Roca; 2000.
15. Matsunaga A, Masuda T, Ogura MN, Saitoh M, Kasahara Y, Iwamura T, et al. Adaptation to low-intensity exercise on a cycle ergometer by patients with acute myocardial infarction undergoing phase I cardiac rehabilitation. Circ J. 2004;68:938-45. [MedLine]
16. Trevisan MD, Myskiw JC. Reabilitação cardiopulmonar e metabólica fase I no pós-operatório de cirurgia de revascularização do miocárdio utilizando cicloergômetro: um ensaio clínico randomizado. 2015; 91p. Acesso em: 14/9/2015. Disponível em: http://repositorio.pucrs.br/dspace/bitstream/10923/7395/1/000470731Texto%2bCompleto-0.pdf.
17. Pires SR, Oliveira AC, Parreira VF, Britto RR. Teste de caminhada de seis minutos em diferentes faixas etárias e índices de massa corporal. Rev Bras Fisioter. 2007;11(2):147-51.
18. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111-7. [MedLine]
19. Arévalo Cárdenas M, García Cardona CG. Respuesta aguda de presión arterial, frecuencia cardíaca y percepción del esfuerzo en hipertensos. Rev Cienc Salud. 2007;5(1):53-66.
20. Fardy PS, Yanowitz FG, Wilson PK. Cardiac rehabilitation, adult fitness, and exercise testing. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 1996. p.55-278.
21. Williams N, Flynn M. A review of the efficacy of neuromuscular electrical stimulation in critically ill patients. Physiother Theory Pract. 2014;30(1):6-11. [MedLine]
22. Burtin C, Clerckx B, Robbeets C, Ferdinande P, Langer D, Troosters T, et al. Early exercise in critically ill patients enhances short-term functional recovery. Crit Care Med. 2009;37(9):2499-505. [MedLine]
23. Dantas CM, Silva PFS, Siqueira FHT, Pinto RMF, Matias S, Maciel C, et al. Influência da mobilização precoce na força muscular periférica e respiratória em pacientes críticos. Rev Bras Ter Intensiva. 2012;24(2):173-8. [MedLine]
No financial support.
Authors' roles & responsibilities
MDT Conception and design; implementation of projects/experiments, final approval of the manuscript
DGCL Conception and design; implementation of projects/experiments, final approval of the manuscript
RGBM Statistical analysis; manuscript writing or critical review of its contents; final approval of the manuscript
FEM Conception and study design; implementation of projects/experiments; analysis and/or interpretation of data; statistical analysis; final approval of the manuscript
AK Analysis/interpretation of data; statistical analysis; final approval of the manuscript
Article receive on Saturday, May 16, 2015
 All scientific articles published at www.rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at www.rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket