![]()
![]()
Fabian Alejandro GómezI; Luis Ernesto BallesterosII; Luz Stella CortésI
DOI: 10.5935/1678-9741.20140101
ABSTRACT
INTRODUCTION: In spite of its importance as an experimental model, the information on the great cardiac vein in pigs is sparse.
OBJECTIVE: To determine the morphologic characteristics of the great cardiac vein and its tributaries in pigs.
METHODS: 120 hearts extracted from pigs destined to the slaughterhouse with stunning method were studied. This descriptive cross-over study evaluated continuous variables with T test and discrete variables with Pearson χ square test. A level of significance P<0.05 was used. The great cardiac vein and its tributaries were perfused with polyester resin (85% Palatal and 15% Styrene) and then subjected to potassium hydroxide infusion to release the subepicardial fat. Calibers were measured, and trajectories and relations with adjacent arterial structures were evaluated.
RESULTS: The origin of the great cardiac vein was observed at the heart apex in 91 (76%) hearts. The arterio-venous trigone was present in 117 (97.5%) specimens, corresponding to the open expression in its lower segment and to the closed expression in the upper segment in the majority of the cases (65%). The caliber of the great cardiac vein at the upper segment of the paraconal interventricular sulcus was 3.73±0.79 mm. An anastomosis between the great cardiac vein and the middle cardiac vein was found in 59 (49%) specimens.
CONCLUSION: The morphological and biometric characteristics of the great cardiac vein and its tributaries had not been reported in prior studies, and due to their similitude with those of the human heart, allows us to propose the pig model for procedural and hemodynamic applications.
RESUMO
INTRODUÇÃO: Apesar de sua importância como um modelo experimental, a informação sobre a grande veia cardíaca em suínos é esparsa.
OBJETIVO: Determinar as características morfológicas da grande veia cardíaca e suas tributárias em suínos.
MÉTODOS: Foram estudados 120 corações extraídos de suínos destinados para o matadouro com método de atordoamento. Este estudo descritivo cross-over avaliou variáveis contínuas com teste T e variáveis discretas com teste χ quadrado de Pearson. O nível de significância P<0,05 foi usado. A grande veia cardíaca e suas tributárias foram perfundidas com resina de poliéster (85% palatal e estireno de 15%) e, em seguida, submetidas à infusão de hidróxido de potássio para remover a gordura subepicardal. Os calibres foram medidos e trajetórias e relações com estruturas arteriais adjacentes foram avaliadas.
RESULTADOS: A origem da grande veia cardíaca foi observada no ápice do coração em 91 (76%) espécimes. O trígono arteriovenoso estava presente em 117 (97,5%) espécimes, correspondente à expressão aberta no seu segmento inferior e para a expressão fechada no segmento superior na maioria dos casos (65%). O calibre da grande veia cardíaca no segmento superior do sulco interventricular paraconal foi de 3,73±0,79 mm. Uma anastomose entre a grande veia cardíaca e da veia cardíaca média foi encontrada em 59 (49%) espécimes.
CONCLUSÃO: As características morfológicas e biométricas da grande veia cardíaca e suas tributárias não haviam sido relatadas em estudos anteriores e, devido à sua semelhança com as do coração humano, nos permite propor o modelo porcino para procedimentos e aplicações hemodinâmicas.
AIB: Anterior interventricular branch
AVT: Arterio-venous trigone of the heart
CBX: Circumflex branch
CS: Coronary sinus
GCV: Great cardiac vein
LAVS: Left atrioventricular sulcus
LCA: Left coronary artery
LMV: Left marginal vein
MCV: Middle cardiac vein
OVLA: Oblique vein of the left atrium
PLCV: Posterior left cardiac vein
RMV: Right marginal vein
INTRODUCTION
Since prior studies have indicated few morphological differences between pigs and humans and since the information available on the venous drainage of the heart is poor, these anatomic characteristics of the pig need to be enriched. The few works conducted on this subject have made vary basic descriptions and have used a limited number of specimens, so the statistic robustness of their findings is debatable[1-3].
The great cardiac vein (GCV) in humans drains into the coronary sinus (CS), the territories irrigated by the left coronary artery (LCA). This vein originates at the lower third of the anterior interventricular sulcus (AIS) or even at the heart apex, and continues its course along said sulcus in parallel to the anterior interventricular branch (AIB) to the upper portion of that artery[4-8]. Then it crosses to the left until it reaches the left atrioventricular sulcus (LAVS) forming the basis of the arterio-venous trigone of the heart (AVT) together with the AIB and the circumflex branch (CxB). Its trajectory is mostly superficial with respect to the artery it runs along with. After a short run through the LAVS, the GCV, receives the drainage of the left posterior veins (PLCV) and gives origin to the SC[4,5,8-15]. The configuration of the AVT of the heart has been based on its crossing or not the GCV to the AIB and the CxB, which determines closed trigones when there is a crossing, or open trigones if the vein does not cross through these arterial branches. The expression of the open AVT in its lower segment and closed AVT in the upper segment have been reported as most frequent (50-73%)[5,8,14,16].
Knowing the cardiac vein system of the pig is useful for experimental anatomic models to train hemodynamists, cardiologists and surgeons[2,3,15,17]. The aim of this study was analyze anatomy of pig cardiac vein and discuss the similarities between these and human cardiac veins.
METHODS
This descriptive cross-over study evaluated the characteristics and main tributaries of the GCV in 120 hearts pigs of commercial breeds destined to the slaughterhouse with stunning method, with a mean age of 5 months. This study was supported by the Bioethics Committee of the Cooperative University of Colombia. The organs were subjected to an exsanguination process in a water source for 6 hours. An arciform plicature was made with silk 2.0 around the CS orifice and a number 14 catheter was installed, through which semisynthetic polyester resin was perfused (palatal GP40L to the 85%; styrene to the 15%) with mineral blue dye. Similarly, prior identification of the ostium and application of a reference point with 2.0 silk, the LCA was perfused with red-stained resin.
Later, the hearts were subjected to a partial corrosion process with 15% potassium hydroxide (KOH) in order to remove the subepicardial fat situated on the bottom of the interventricular and atrioventricular sulci. Then, the GCV and its tributaries were dissected from their origin to their distal segment. The caliber of the GCV was measured with an electronic calibrator (Mitutoyo®), at its upper interventricular and atrio-ventricular segments and at its end. The GCV tributaries were measured at their medium and distal segments. The presence of a venous communication of the GCV with other venous branches was determined. The superficial or deep relation of the GCV with respect to the paraconal interventricular branch (PIB) was established, as well as the trajectories parallel to the right or left and the proximal or distal crossings of the GCV with respect to the PIB. The configuration of the AVT of the heart determined by the relation of the GCV with the branches of the LCA, PIB and CxB were classified according to Pejkovic & Bogdanovic[10] criteria; as opened in its lower segment and closed in its upper segment; both lower and upper opened; both lower and upper closed; lower closed and upper opened.
The data thus obtained were recorded in a physical matrix and were consigned in digital media using Excel tables. Photographs were taken to each one of the pieces evaluated with digital camera. Continuous variables were described with means and standard deviation, nominal variables with proportions.
RESULTS
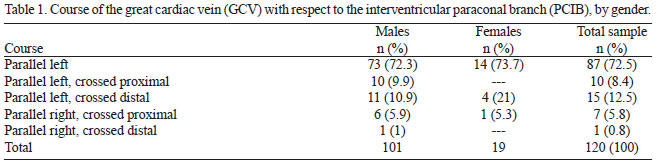
One hundred and twenty hearts were evaluated, 101 (84.2%) of which were from male pigs and 19 (15.8%) from female pigs. The mean weight of the hearts was 375±78.12 g. The specimens were obtained from pigs with a mean weight of 90 kg and between 4 and 5 months of age. In 91 (76%) hearts the GCV originated at the heart apex and in 29 (24%) at the lower third of the sternocostal surface of the heart. This vessel showed a left parallel course with respect to the PIB in 87 (72.5%) specimens and a right parallel trajectory with distal crossing in 1 (0.8%) case (Table 1).
The AVT was present in 117 (97.5%) specimens. In the cases in which it was absent, the GCV took an ascending course crossing the proximal segment of the CxB, going then to the left of the ascending aorta, and finally draining into the right atrium above the outlet of the CS (2.5%). In these 3 cases the CS received the drainage of the left marginal vein (LMV), of the PLCV and the middle cardiac vein (MCV) (Figure 1).

An open configuration of the AVT at the lower portion and closed at the upper portion was observed in 76 (65%) cases (Figure 2); closed in both its lower and upper segments in 20 (17%) especimens (Figure 3); open in its lower and upper portions in 15 (13%) hearts (Figure 4), and closed at its lower portion and open at its upper portion in 6 (5%) specimens (Figure 5).




The caliber of the GCV at the paraconal interventricular sulcus was 3.73±0.79 mm; at the LAVS it was 4.99±1.04 mm, and at the site of drainage into the coronary sinus was 5.3±0.98 mm. The GCV received on average the drainage of 3.5 right anterior ventricular branches and 5.5 left anterior ventricular branches and in 99% of the cases it was superficial with respect to the PIB. A venous communication between the GCV and the MCV was found in 59 (49%) specimens (Figure 6) and with the right marginal vein (RMV) in 2 (1.5%) cases.

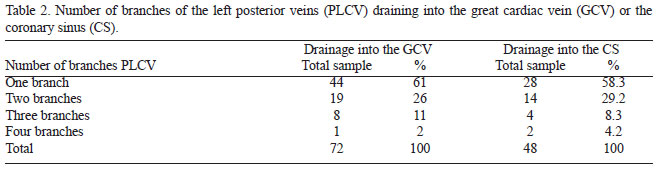
The PLCVs had a caliber of 1.61±0.61 mm and drained into the GCV in 58% of the cases, and into the CS in 42% (Figure 7). One to four branches drained into each one of these structures, with a predominance of the expression of a single branch (Table 2).

The LMV was originated at the heart apex in 54 (46%) specimens, and at the middle third of the obtuse edge of the heart in 30%; whereas in 16 (14%) hearts this structure was originated at the lower third and was very short, having its origin at the upper third in 12 (10%) cases. The LMV drained into the distal segment of the GCV in 116 (97%) specimens and into the proximal segment of the CS in 3 (2.5%) specimens; in one case it drained into an anterior ventricular branch (0.5%). The mean caliber of the LMV was 1.53±0.51 mm and the distal caliber was 2.61±0.75 mm.
DISCUSSION
There are no data from pigs on the caliber and length of the GCV; most prior studies have only limited to describe its qualitative characteristics[1,2]. With respect to the GCV originating mostly at the heart apex, our findings are consistent with reports in humans, but while the frequency in our series is of 76%, in humans it has been reported in a range of 27-57.4%[6,8,18,19]. In 24% of the cases the GCV originated at the lower third of the paraconal interventricular sulcus coinciding with some studies in humans[6,19]. Some other authors have reported the origin of the GCV at this level with a greater frequency, within a range of 57-74%[5,9,11]. When this anatomic expression occurs, the venous drainage is compensated with the finding of a long MCV originating at the lower third of the anterior ventricular surface.
The location of the GCV to the left of the PIB of the LCA observed in our series in 93% of the specimens exceeds what has been reported in humans[8], with this characteristic being determinant for the high percentage of open forms of the lower segment of the AVT. The characterization of the trajectory of the GCV in parallel to the PIB, together with the proximal or distal crossings of the vein over the artery where it runs along with, is new information on anatomy of the GCV in pigs and are useful for procedures using this animal model.
In our study a few specimens of the GCV ran along the PIB until the vicinity to the point of division of the LCA, without giving place to the formation of the cardiac AVT as classically described. The high incidence of the AVT in our series (97.5%) is considerably greater than that reported in humans (59-80%)[5,8,11,12,16,20]. The absence of an AVT could hamper the pass of electrodes during radiofrequency ablation procedures utilized for the management of heart failure due to foci of arrhythmia[9]. Similarly, our findings are consistent with those reported in human heartsindicating an open expression of the TAV inferiorly as the most frequent, although the frequency observed in our sample was slightly higher (65%)[5,8,16]. In our series the incidence of the open form of the upper and lower segments of cardiac AVT (13%) was similar to the study by Ortale et al.[5], and slightly higher than the reports by other authors[8,16].
In humans the superficial location of the GCV with respect to the AIB of the LCA has been reported within a range of between 60-85%, consistent with our findings where the vein runs superficially to the PIB, but its frequency (99%) is superior to what has been reported in humans[8,9,11,12]. This situation in humans has been considered relevant because in the presence of occlusive coronary heart disease cases where the GCV runs deeply in the AVT this vessel could be compressed by rigid arteries that would alter the venous return of the heart and would worsen the disease[16,20].
The mean calibers of the GCV found in our study at the interventricular sulcus and at the distal segment (3.73 mm and 5.3 mm, respectively), are consistent with the majority of the reports from studies in humans[4,9,16,21,22].
The venous communication found between the GCV and the MCV at the heart apex (49%) in our study, is considerably more numerous than those reported in humans indicating ranges between 15-34%[5,8,9,11,14,16]. Melo et al.[4], in a study conducted in humans, reported venous communication of these veins in 90% of the cases, although they do not discriminate where these venous communication occurred. This morphological characteristic has been considered as protective because in certain pathophysiologic conditions allow to attenuate or prolong the history of the cardiovascular disease by providing alternative routes for venous drainage[8].
The caliber of the LMV reported in prior studies in humans[5,8,11,21] is similar to our findings (2.61 mm). Concerning the drainage of the LMV, our results are consistent with reports in humans indicating this vascular structure draining into the GCV in the majority of the cases, but there is some controversy about the frequency of its drainage into the CS, which was found in our study in 2.5%, whereas in humans it has been reported within a range of 5-19%[5,8,11]. The findings about the qualitative and morphometric characteristics of the LMV are new knowledge that had not been previously described in the literature.
The drainage of the PLCV in the GCV had been described in humans in a range of 28-35%, whereas in our study we observed in 42% of the specimens. Similarly, our findings are consistent with those of prior studies conducted in humans, with respect to the caliber and the prevalent expression of one or two PLCV at their turn receiving small tributaries that drained the lateral and posterior surface of the left ventricle, then to drain into the GCV or into the CS[7,8,13,15]. The large variations in number of the PLCV should be taken into account for the insertion of devices in the management of arrhythmias; the absence of the lateral veins or the small number of PLCV, may virtually limit the possibility of going into the left ventricle through a venous access. The dimensions of the PLCV, have a negative correlation with its number, which leads to the high number of tributaries, the lower the accessibility with the available catheters, so that these characteristics become relevant in the practice of intravenous approaches to the heart[5,6]. Interventionist cardiologists consider that the minimum diameter of these vessels for an appropriate manipulation with an intracoronary mapping catheter should be 1.3 mm, because the diameter of the devices is 1.1 mm[3,4]. The mean caliber of the PLCV found in our series (1.61 mm) allows us to propose to the young adult pig model as a good training scenario for the application of intravenous devices through the GCV and its left posterior ventricular tributaries.
CONCLUSION
The morphological and biometric characteristics of the GCV and its tributaries in pigs had not been reported in prior studies, similitudes of GCV anatomy in pigs enable the use of pig hearts as models for surgical and hemodynamics procedures.
ACKNOWLEDGEMENTS
To Frigorífico Vijagual in the city of Bucaramanga - Colombia for the donation of pieces to conduct this investigation and to the students Diana Reyes and Jairo Rivera, for their participation in the preparation of the study specimens.
REFERENCES
1. Kato T, Yasue T, Shoji Y, Shimabukuro S, Ito Y, Goto S, et al. Angiographic difference in coronary artery of man, dog, pig and monkey. Acta Pathol Jpn. 1987;37(3):361-73. [MedLine]
2. Crick SJ, Sheppard MN, Ho SY, Gebstein L, Anderson RH. Anatomy of the pig heart: comparisons with normal human cardiac structure. J Anat. 1998;193(Pt 1):105-19. [MedLine]
3. Sahni D, Kaur GD, Jit H, Jit I. Anatomy & distribution of coronary arteries in pig in comparison with man. Indian J Med Res. 2008;127(6):564-70. [MedLine]
4. Melo DS, Prudencio LA, Kusnir CE, Pereira AL, Marques V, Vieira MC, et al. Angiography of the coronary venous system. Use in clinical electrophysiology. Arq Bras Cardiol. 1998;70(6):409-13. [MedLine]
5. Ortale JR, Gabriel EA, Iost C, Márquez CQ. The anatomy of the coronary sinus and its tributaries. Surg Radiol Anat. 2001;23(1):15-21. [MedLine]
6. El-Maasarany S, Ferrett CG, Firth A, Sheppard M, Henein MY. The coronary sinus conduit function: anatomical study (relationship to adjacent structures). Europace. 2005;7(5):475-81. [MedLine]
7. Sousa-Rodrigues CF, Alcântara FS, Olave E. Topografía y biometría del sistema venoso coronario y de sus tributarias. Int J Morphol. 2005;23:177-84.
8. Ballesteros LE, Ramírez LM, Forero PL. Study of the coronary sinus and its tributaries in Colombian subjects. Rev Colomb Cardiol. 2010;17(1):9-15.
9. Mochizuki S. Vv. Cordis. In: Adachi B, eds. Das venensystem der Japaner. Kyoto: Kenkyusha; 1933. p.41-64.
10. Pejkovic B, Bogdanovic D. The great cardiac vein. Surg Radiol Anat. 1992;14(1):23-8. [MedLine]
11. Mahmud E, Raisinghani A, Keramati S, Auger W, Blanchard DG, DeMaria AN. Dilation of the coronary sinus on echocardiogram: prevalence and significance in patients with chronic pulmonary hypertension. J Am Soc Echocardiogr. 2001;14(1):44-9. [MedLine]
12. Liu DM, Zhang FH, Chen L, Zheng HP, Zhong SZ. Anatomy of the coronary sinus and its clinical significance for retrograde cardioplegia. Di Yi Jun Yi Da Xue Xue Bao. 2003;23(4):358-60.
13. Piffer CR, Piffer MI, Zorzetto NL. Anatomic data of the human coronary sinus. Anat Anz. 1990;170(1):21-9. [MedLine]
14. Kaczmarek M, Czerwinski F. Assessment of the course of the great cardiac vein in a selected number of human hearts. Folia Morphol (Warsz). 2007;66(3):190-3. [MedLine]
15. Schlesinger MJ. Relation of anatomic pattern to pathologic conditions of the coronary arteries. Arch Pathol. 1940;30:403-15.
16. von Lüdinghausen M. Clinical anatomy of cardiac veins, Vv. cardiacae. Surg Radiol Anat. 1987;9(2):159-68. [MedLine]
17. Lee MS, Shah AP, Dang N, Berman D, Forrester J, Shah PK, et al. Coronary sinus is dilated and outwardly displaced in patients with mitral regurgitation: quantitative angiographic analysis. Catheter Cardiovasc Interv. 2006;67(3):490-4. [MedLine]
18. Schaffler GJ, Groell R, Peichel KH, Rienmüller R. Imaging the coronary venous drainage system using electron-beam CT. Surg Radiol Anat. 2000;22(1):35-9. [MedLine]
19. Christiaens L, Ardilouze P, Ragot S, Mergy J, Allal J. Prospective evaluation of the anatomy of the coronary venous system using multidetector row computed tomography. Int J Cardiol. 2008;126(2):204-8. [MedLine]
20. Kawashima T, Sato K, Sato F, Sasaki H. An anatomical study of the human cardiac veins with especial reference to the drainage of the great cardiac vein. Ann Anat. 2003;185(6):535-42. [MedLine]
21. Gilard M, Mansourati J, Etienne Y, Larlet JM, Truong B, Boschat J, et al. Angiographic anatomy of the coronary sinus and its tributaries. Pacing Clin Electrophysiol. 1998;21(11 Pt 2):2280-4. [MedLine]
No financial support
Authors' roles & responsibilities
FAG: Analysis and/or interpretation of data, statistical analysis, final approval of the manuscript, conception and design of the study, implementation of operations and/or experiments, manuscript writing or critical review of its content
LEB: Analysis and/or interpretation of data, statistical analysis, final approval of the manuscript, conception and design of the study, implementation of operations and/or experiments, manuscript writing or critical review of its content
LSC: Conception and design of the study, implementation of operations and/or experiments, manuscript writing or critical review of its content
Article receive on Tuesday, June 24, 2014
 All scientific articles published at www.rbccv.org.br are licensed under a Creative Commons license
All scientific articles published at www.rbccv.org.br are licensed under a Creative Commons license













All rights reserved 2017 / © 2024 Brazilian Society of Cardiovascular Surgery
DEVELOPMENT BY ![]()
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket